This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
4 Citations 9 Q&As





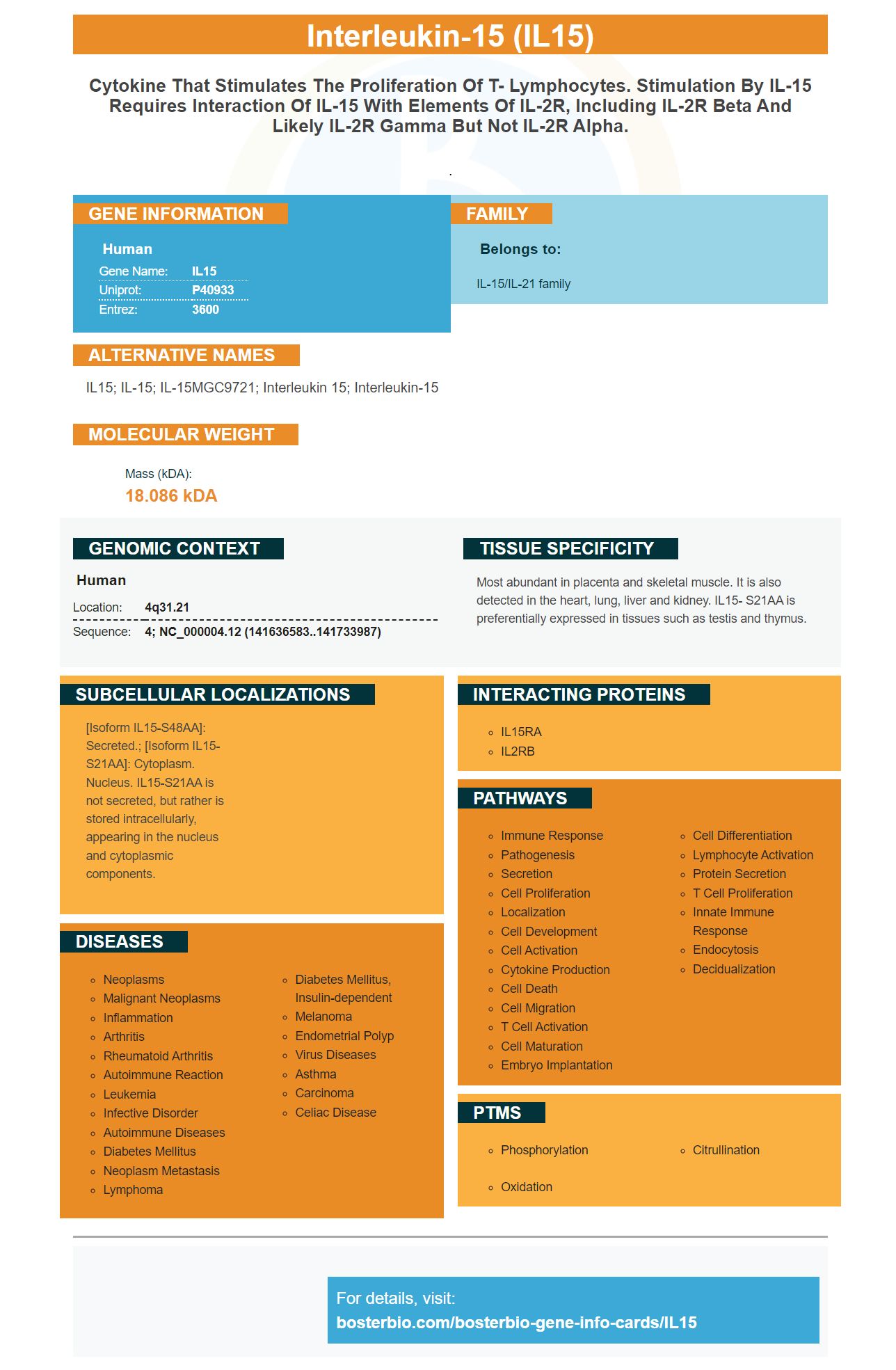
Facts about Interleukin-15.

.
| Human | |
|---|---|
| Gene Name: | IL15 |
| Uniprot: | P40933 |
| Entrez: | 3600 |

| Belongs to: |
|---|
| IL-15/IL-21 family |

IL15; IL-15; IL-15MGC9721; interleukin 15; interleukin-15
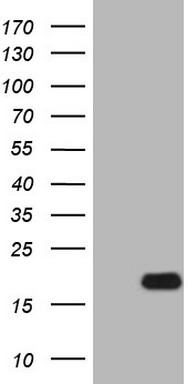
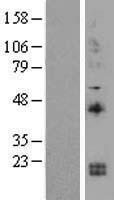
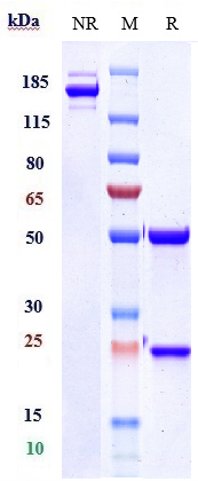
Mass (kDA):
18.086 kDA

| Human | |
|---|---|
| Location: | 4q31.21 |
| Sequence: | 4; NC_000004.12 (141636583..141733987) |
Most abundant in placenta and skeletal muscle. It is also detected in the heart, lung, liver and kidney. IL15- S21AA is preferentially expressed in tissues such as testis and thymus.
[Isoform IL15-S48AA]: Secreted.; [Isoform IL15-S21AA]: Cytoplasm. Nucleus. IL15-S21AA is not secreted, but rather is stored intracellularly, appearing in the nucleus and cytoplasmic components.




PMID: 8178155 by Grabstein K.H., et al. Cloning of a T cell growth factor that interacts with the beta chain of the interleukin-2 receptor.
PMID: 8932977 by Krause H., et al. Genomic sequence and chromosomal location of the human interleukin-15 gene (IL15).
*More publications can be found for each product on its corresponding product page