This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
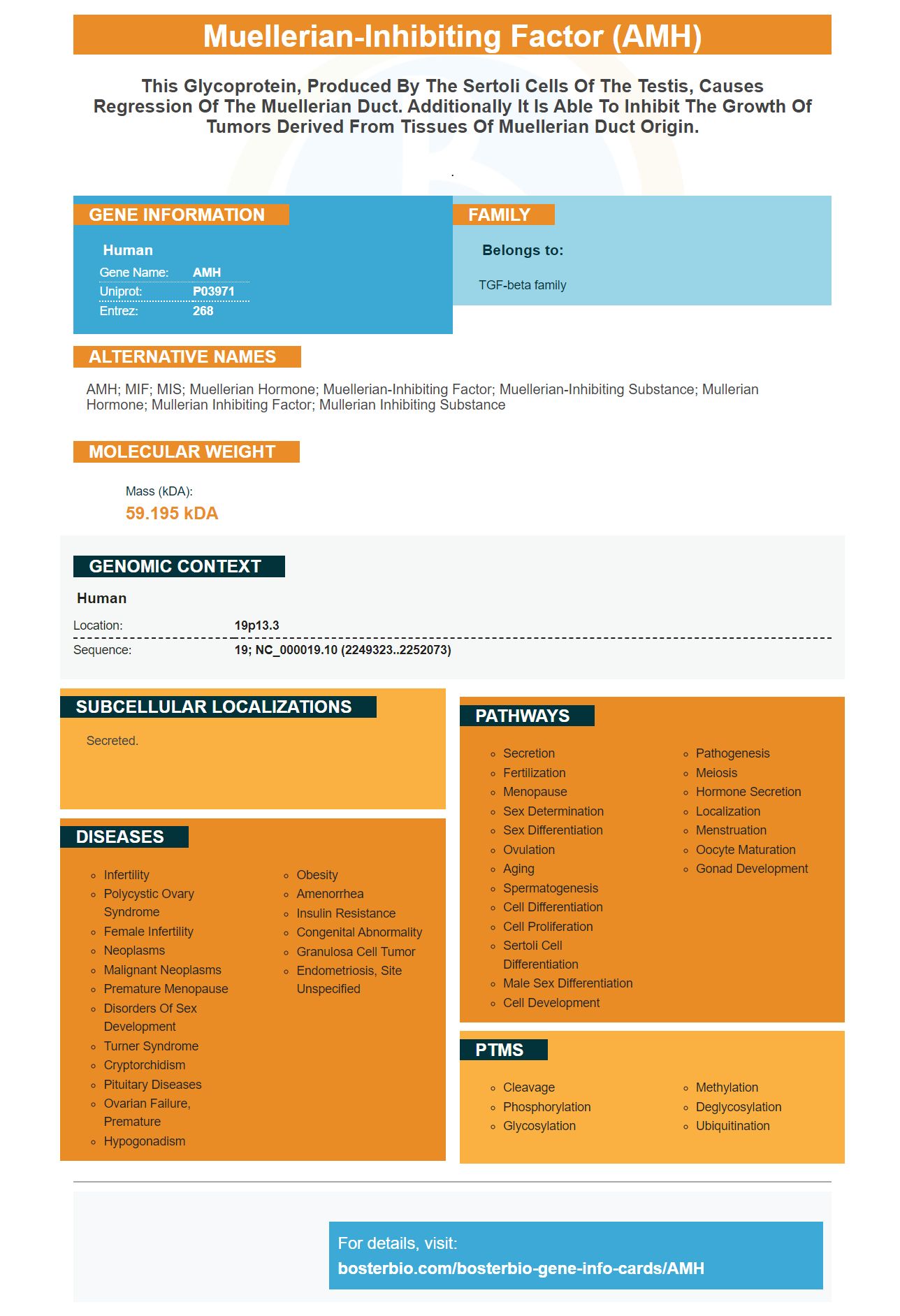
Facts about Muellerian-inhibiting factor.

.
| Human | |
|---|---|
| Gene Name: | AMH |
| Uniprot: | P03971 |
| Entrez: | 268 |

| Belongs to: |
|---|
| TGF-beta family |

AMH; MIF; MIS; Muellerian hormone; muellerian-inhibiting factor; muellerian-inhibiting substance; Mullerian hormone; Mullerian inhibiting factor; Mullerian inhibiting substance
Mass (kDA):
59.195 kDA

| Human | |
|---|---|
| Location: | 19p13.3 |
| Sequence: | 19; NC_000019.10 (2249323..2252073) |
Secreted.



PMID: 3754790 by Cate R.L., et al. Isolation of the bovine and human genes for Mullerian inhibiting substance and expression of the human gene in animal cells.
PMID: 1483695 by Carre-Eusebe D., et al. Variants of the anti-Mullerian hormone gene in a compound heterozygote with the persistent Mullerian duct syndrome and his family.