This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
2 Citations


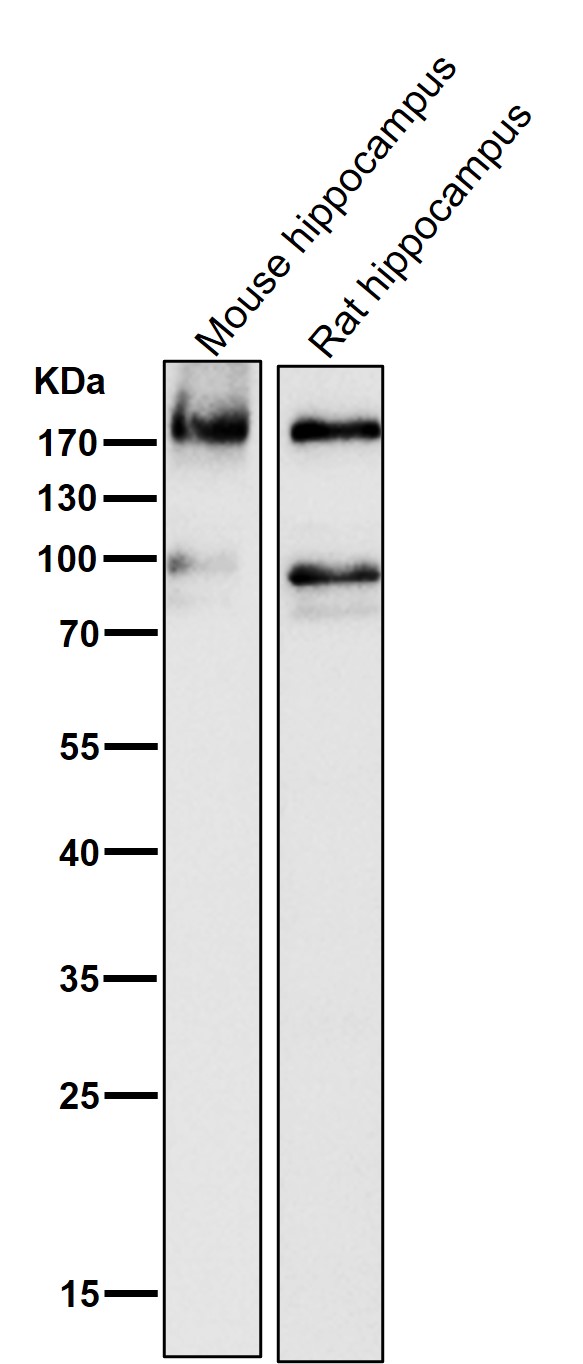
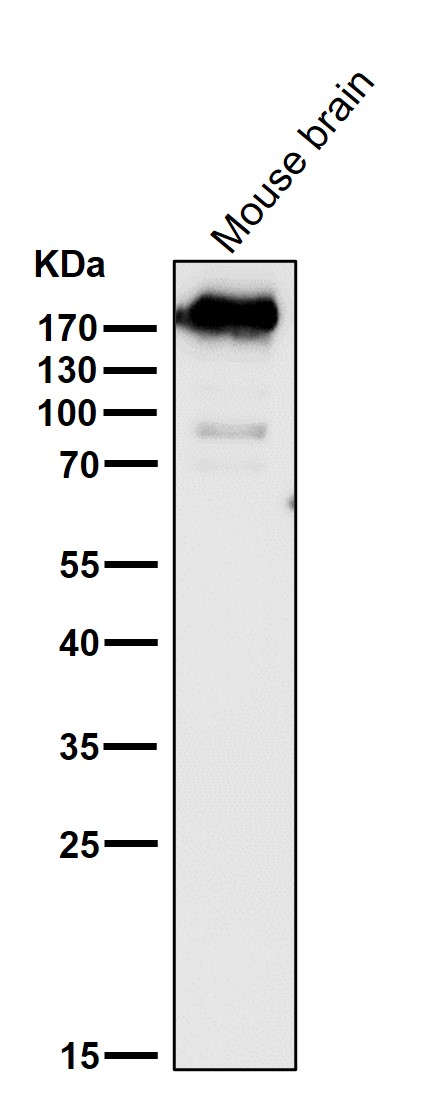
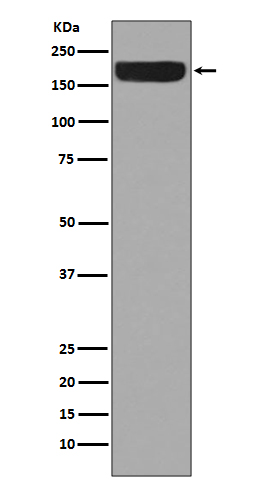
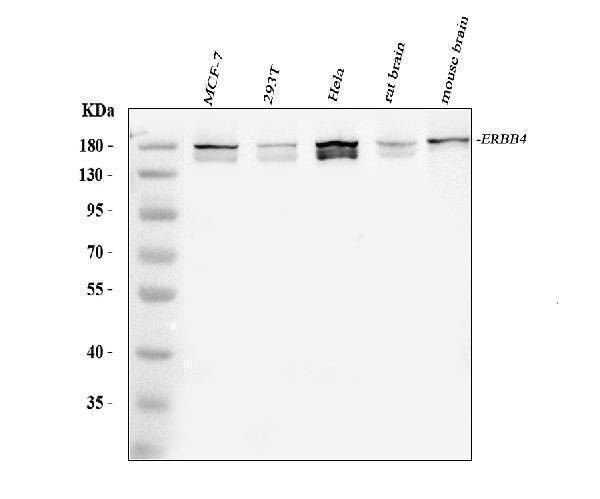
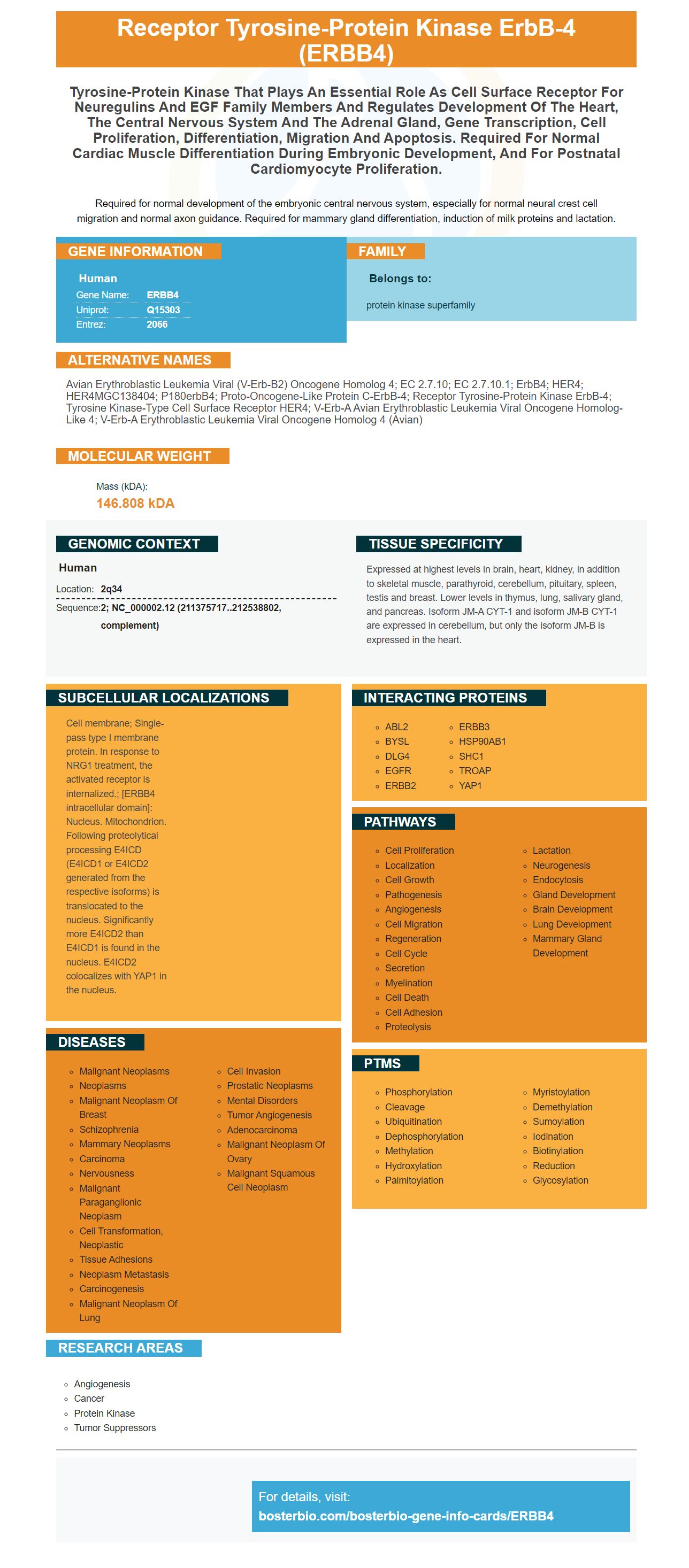
Facts about Receptor tyrosine-protein kinase erbB-4.

Required for normal development of the embryonic central nervous system, especially for normal neural crest cell migration and normal axon guidance. Required for mammary gland differentiation, induction of milk proteins and lactation.
| Human | |
|---|---|
| Gene Name: | ERBB4 |
| Uniprot: | Q15303 |
| Entrez: | 2066 |

| Belongs to: |
|---|
| protein kinase superfamily |

avian erythroblastic leukemia viral (v-erb-b2) oncogene homolog 4; EC 2.7.10; EC 2.7.10.1; ErbB4; HER4; HER4MGC138404; p180erbB4; Proto-oncogene-like protein c-ErbB-4; receptor tyrosine-protein kinase erbB-4; Tyrosine kinase-type cell surface receptor HER4; v-erb-a avian erythroblastic leukemia viral oncogene homolog-like 4; v-erb-a erythroblastic leukemia viral oncogene homolog 4 (avian)
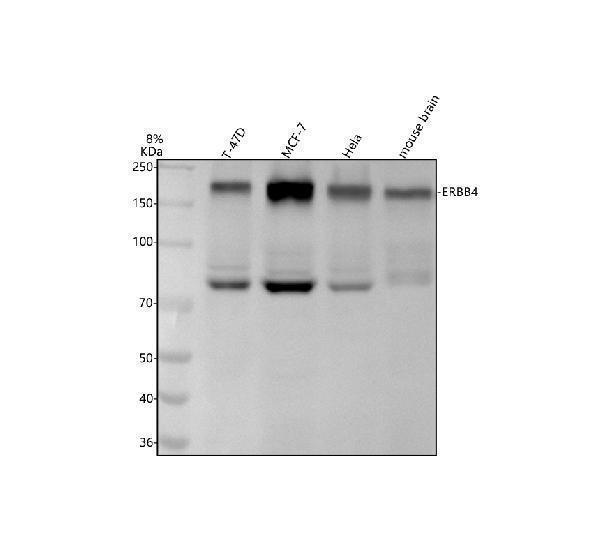
Mass (kDA):
146.808 kDA

| Human | |
|---|---|
| Location: | 2q34 |
| Sequence: | 2; NC_000002.12 (211375717..212538802, complement) |
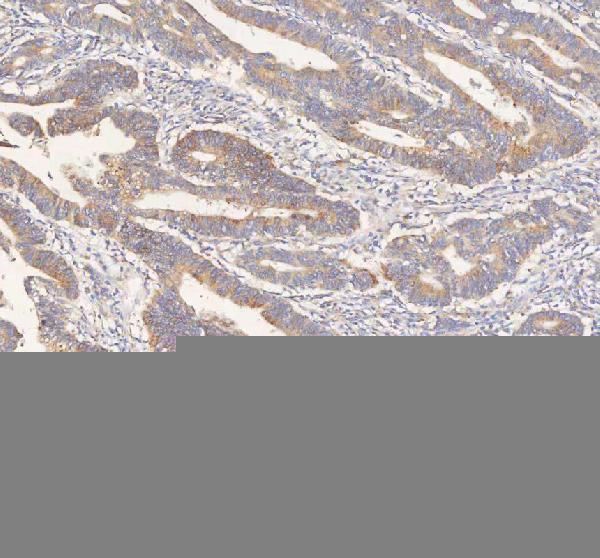
Expressed at highest levels in brain, heart, kidney, in addition to skeletal muscle, parathyroid, cerebellum, pituitary, spleen, testis and breast. Lower levels in thymus, lung, salivary gland, and pancreas. Isoform JM-A CYT-1 and isoform JM-B CYT-1 are expressed in cerebellum, but only the isoform JM-B is expressed in the heart.
Cell membrane; Single-pass type I membrane protein. In response to NRG1 treatment, the activated receptor is internalized.; [ERBB4 intracellular domain]: Nucleus. Mitochondrion. Following proteolytical processing E4ICD (E4ICD1 or E4ICD2 generated from the respective isoforms) is translocated to the nucleus. Significantly more E4ICD2 than E4ICD1 is found in the nucleus. E4ICD2 colocalizes with YAP1 in the nucleus.




PMID: 8383326 by Plowman G.D., et al. Ligand-specific activation of HER4/p180erbB4, a fourth member of the epidermal growth factor receptor family.
PMID: 9334263 by Elenius K., et al. A novel juxtamembrane domain isoform of HER4/ErbB4. Isoform-specific tissue distribution and differential processing in response to phorbol ester.