This website uses cookies to ensure you get the best experience on our website.
- Table of Contents

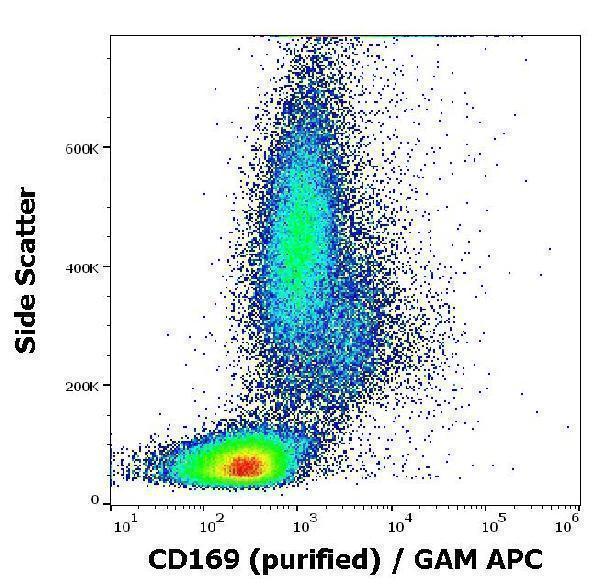


Facts about Sialoadhesin.

Preferentially binds to alpha-2,3-linked sialic acid (By similarity). Binds to SPN/CD43 on T-cells (By similarity).
| Human | |
|---|---|
| Gene Name: | SIGLEC1 |
| Uniprot: | Q9BZZ2 |
| Entrez: | 6614 |

| Belongs to: |
|---|
| immunoglobulin superfamily |

CD169; FLJ00051; sialic acid binding Ig-like lectin 1, sialoadhesin; sialoadhesin; Siglec1; Siglec-1
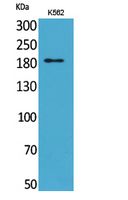
Mass (kDA):
182.624 kDA

| Human | |
|---|---|
| Location: | 20p13 |
| Sequence: | 20; NC_000020.11 (3686970..3712600, complement) |
Expressed by macrophages in various tissues. High levels are found in spleen, lymph node, perivascular macrophages in brain and lower levels in bone marrow, liver Kupffer cells and lamina propria of colon and lung. Also expressed by inflammatory macrophages in rheumatoid arthritis.
[Isoform 1]: Cell membrane; Single-pass type I membrane protein.; [Isoform 2]: Secreted.



PMID: 11133773 by Hartnell A., et al. Characterization of human sialoadhesin, a sialic acid binding receptor expressed by resident and inflammatory macrophage populations.
PMID: 11214971 by Hattori A., et al. Characterization of long cDNA clones from human adult spleen.