This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
3 Citations 8 Q&As

Facts about Securin.

Throughout the mitosis, it blocks Separase/ESPL1 function, preventing the proteolysis of the cohesin complex and the subsequent segregation of the chromosomes. At the onset of anaphase, it's ubiquitinated, conducting to its destruction and to the liberation of ESPL1.
| Human | |
|---|---|
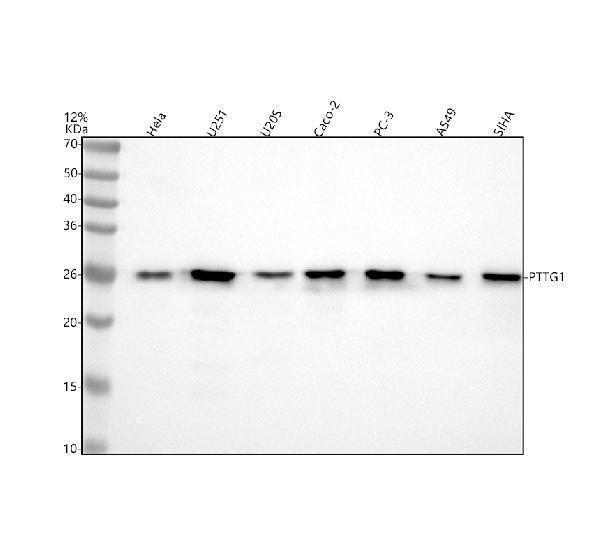
| Gene Name: | PTTG1 |
| Uniprot: | O95997 |
| Entrez: | 9232 |

| Belongs to: |
|---|
| securin family |

EAP1MGC126883; ESP1-associated protein 1; Esp1-associated protein; hPTTG; pituitary tumor-transforming 1; Pituitary tumor-transforming gene 1 protein; PTTGMGC138276; securin; Tumor-transforming protein 1; TUTR1HPTTG
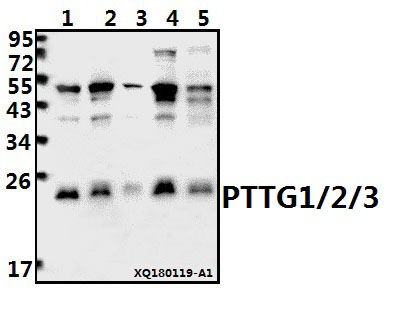
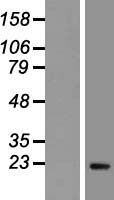
Mass (kDA):
22.024 kDA

| Human | |
|---|---|
| Location: | 5q33.3 |
| Sequence: | 5; NC_000005.10 (160421855..160428744) |
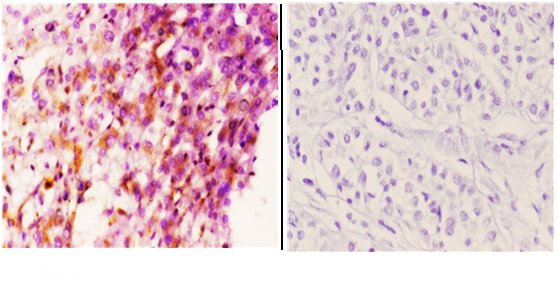
Expressed at low level in most tissues, except in adult testis, where it is highly expressed. Overexpressed in many patients suffering from pituitary adenomas, primary epithelial neoplasias, and esophageal cancer.
Cytoplasm. Nucleus.



PMID: 9811450 by Dominguez A., et al. hPTTG, a human homologue of rat PTTG, is overexpressed in hematopoietic neoplasms. Evidence for a transcriptional activation function of hPTTG.
PMID: 10393434 by Kakar S.S., et al. Molecular cloning and characterization of the tumor transforming gene (TUTR1): a novel gene in human tumorigenesis.
*More publications can be found for each product on its corresponding product page