This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
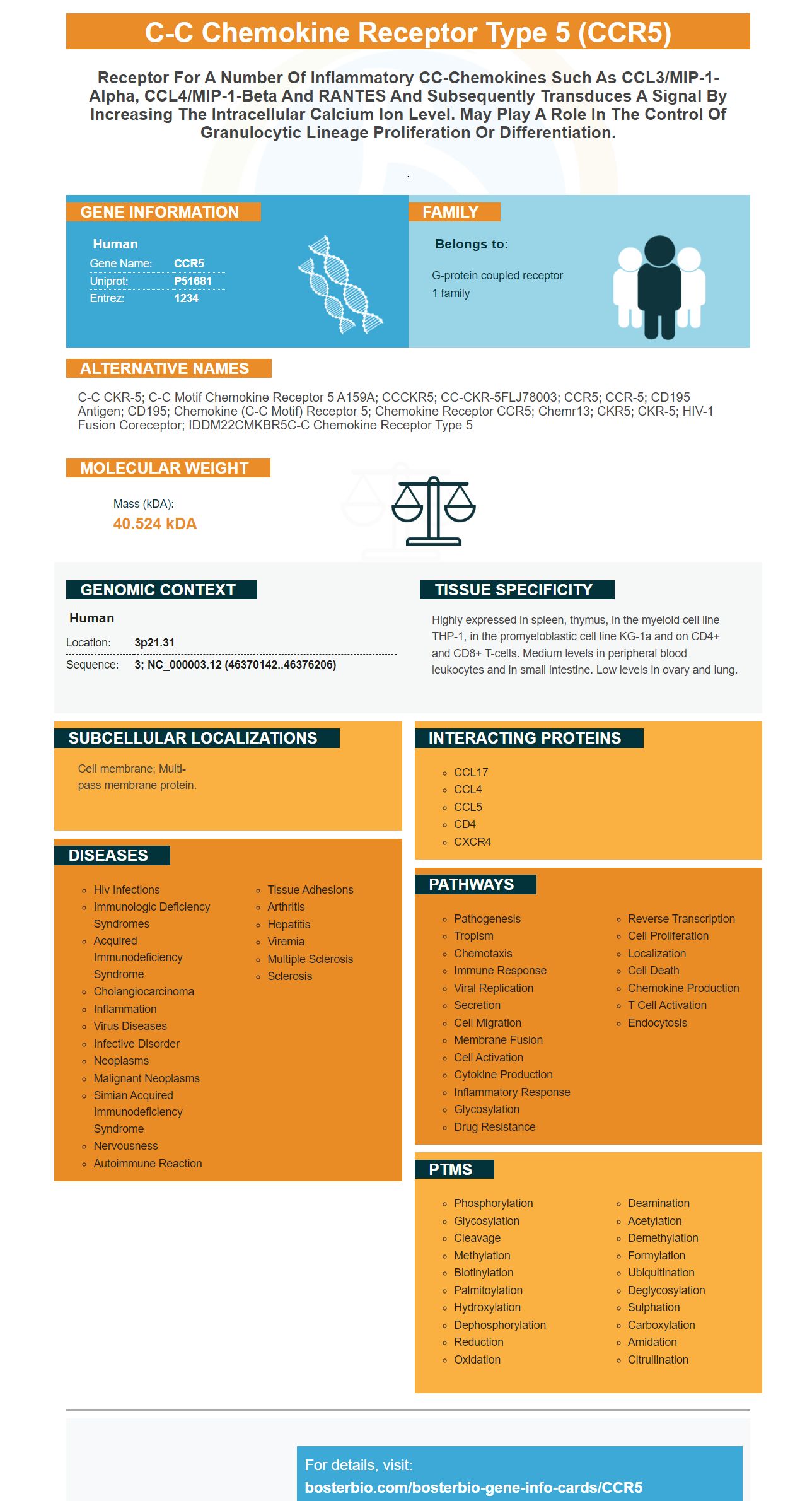




Facts about C-C chemokine receptor type 5.

.
| Human | |
|---|---|
| Gene Name: | CCR5 |
| Uniprot: | P51681 |
| Entrez: | 1234 |

| Belongs to: |
|---|
| G-protein coupled receptor 1 family |

C-C CKR-5; C-C motif chemokine receptor 5 A159A; CCCKR5; CC-CKR-5FLJ78003; CCR5; CCR-5; CD195 antigen; CD195; chemokine (C-C motif) receptor 5; chemokine receptor CCR5; chemr13; CKR5; CKR-5; HIV-1 fusion coreceptor; IDDM22CMKBR5C-C chemokine receptor type 5
Mass (kDA):
40.524 kDA

| Human | |
|---|---|
| Location: | 3p21.31 |
| Sequence: | 3; NC_000003.12 (46370142..46376206) |
Highly expressed in spleen, thymus, in the myeloid cell line THP-1, in the promyeloblastic cell line KG-1a and on CD4+ and CD8+ T-cells. Medium levels in peripheral blood leukocytes and in small intestine. Low levels in ovary and lung.
Cell membrane; Multi-pass membrane protein.




PMID: 8639485 by Samson M., et al. Molecular cloning and functional expression of a new human CC- chemokine receptor gene.
PMID: 8663314 by Raport C.J., et al. Molecular cloning and functional characterization of a novel human CC chemokine receptor (CCR5) for RANTES, MIP-1beta, and MIP-1alpha.
*More publications can be found for each product on its corresponding product page