This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
54 Citations 16 Q&As
193 Citations 16 Q&As
59 Citations 16 Q&As
25 Citations 18 Q&As
1 Citations 16 Q&As
28 Citations 4 Q&As
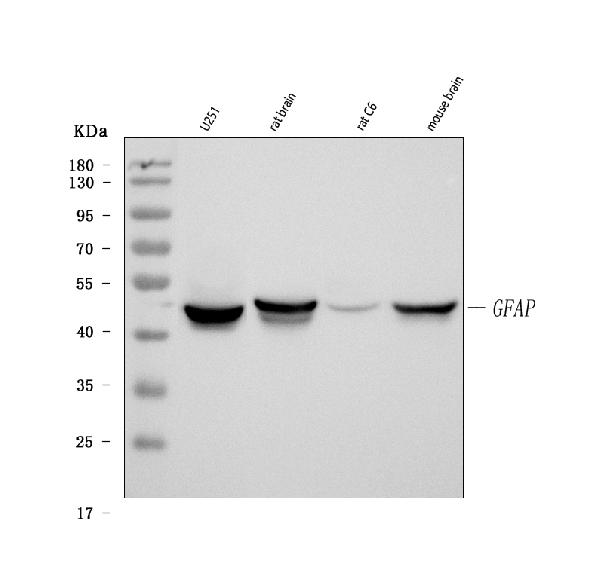
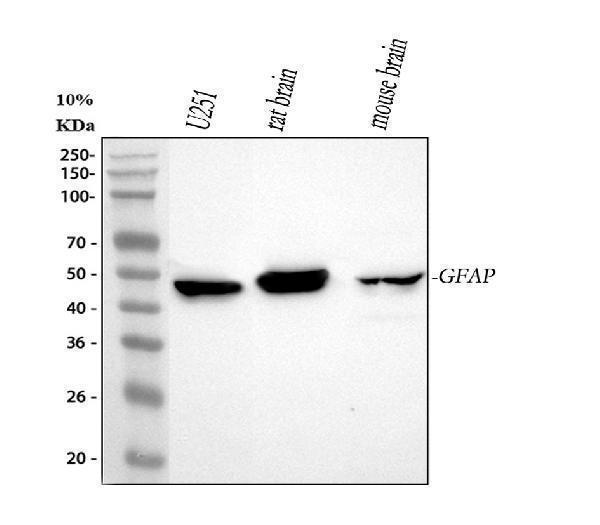
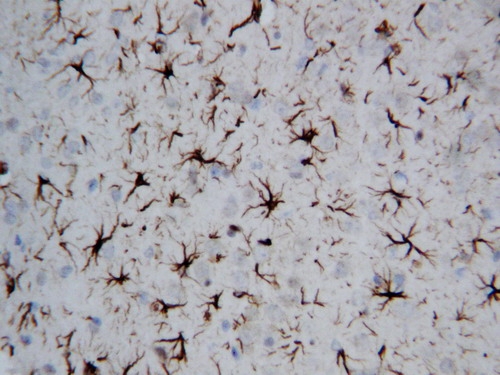
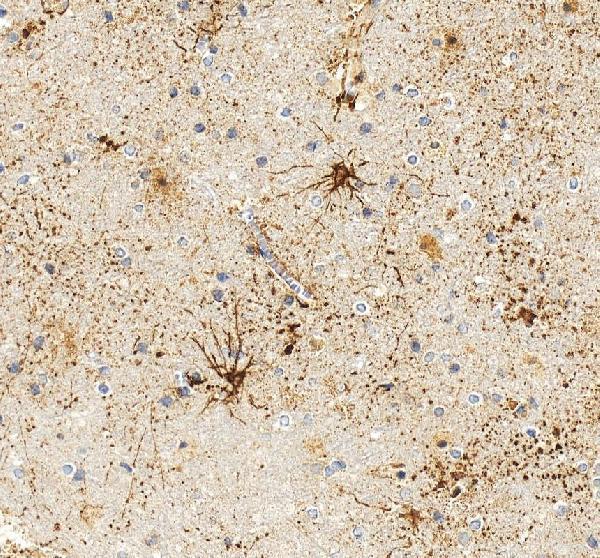
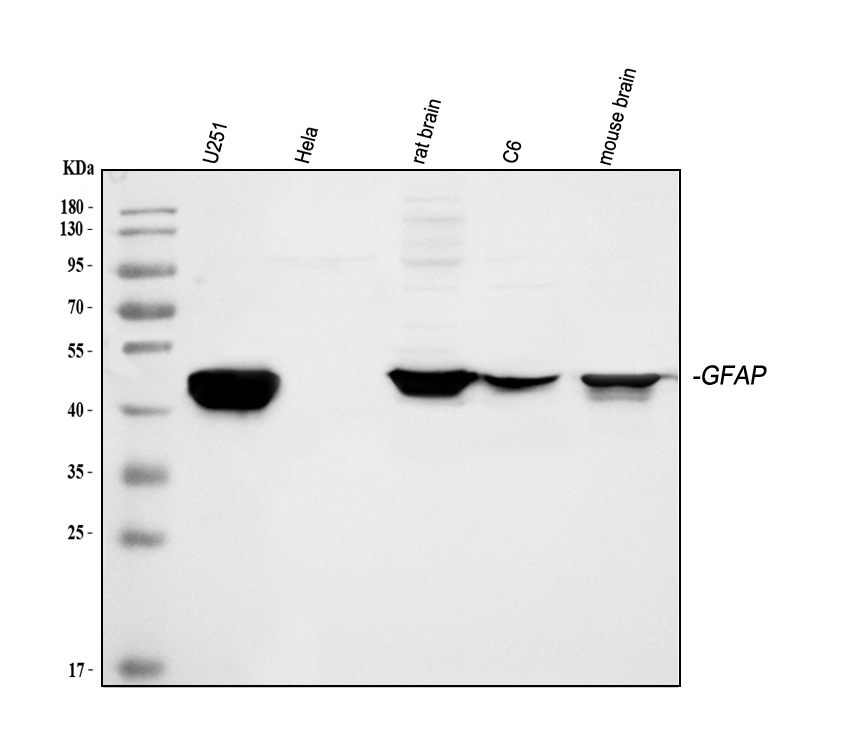
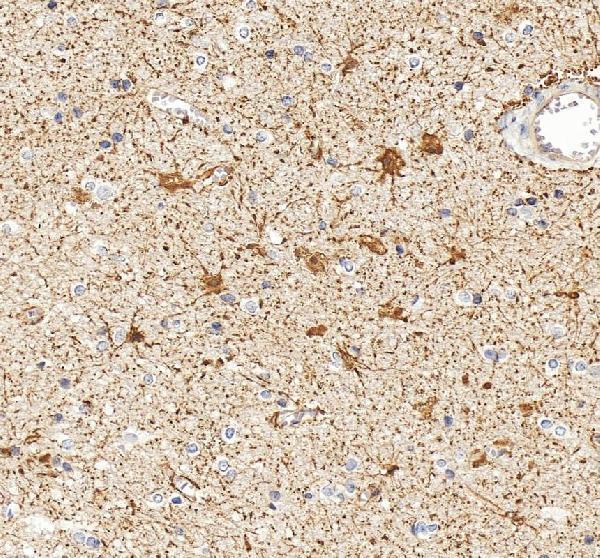
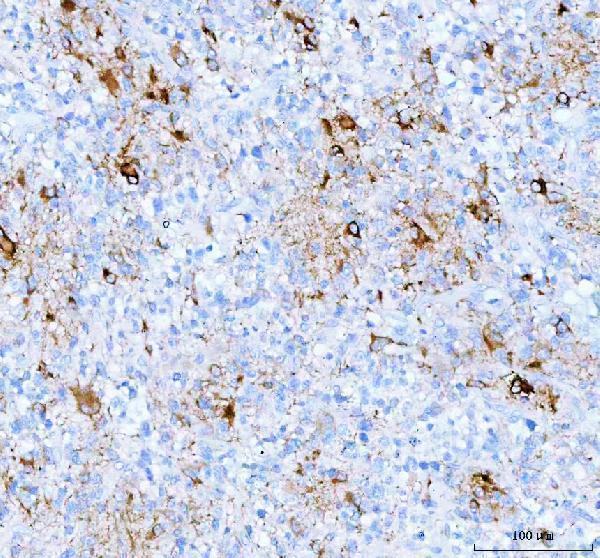
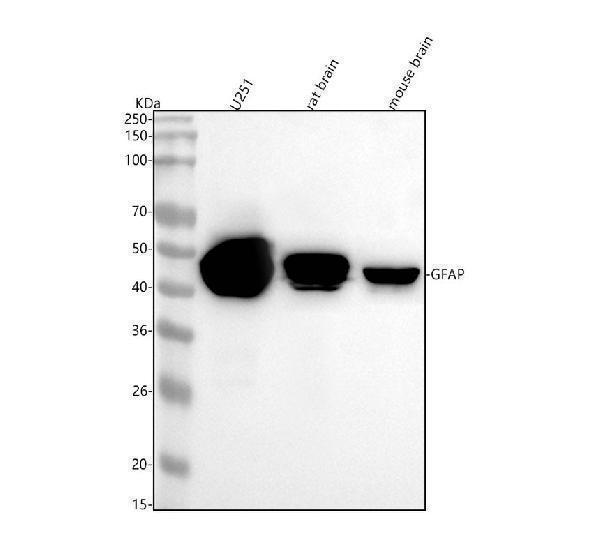
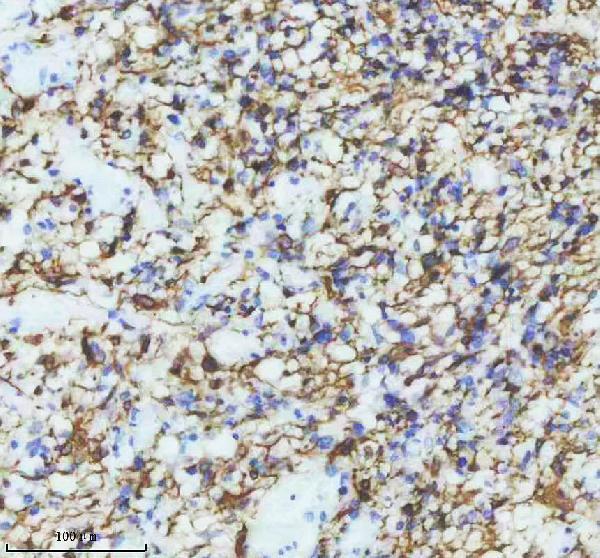
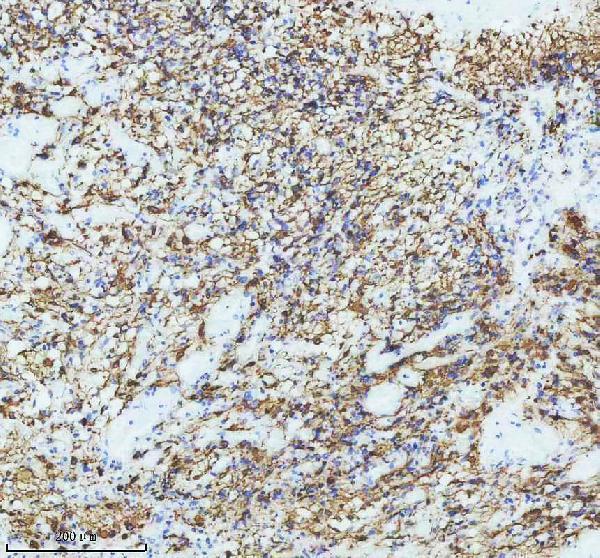
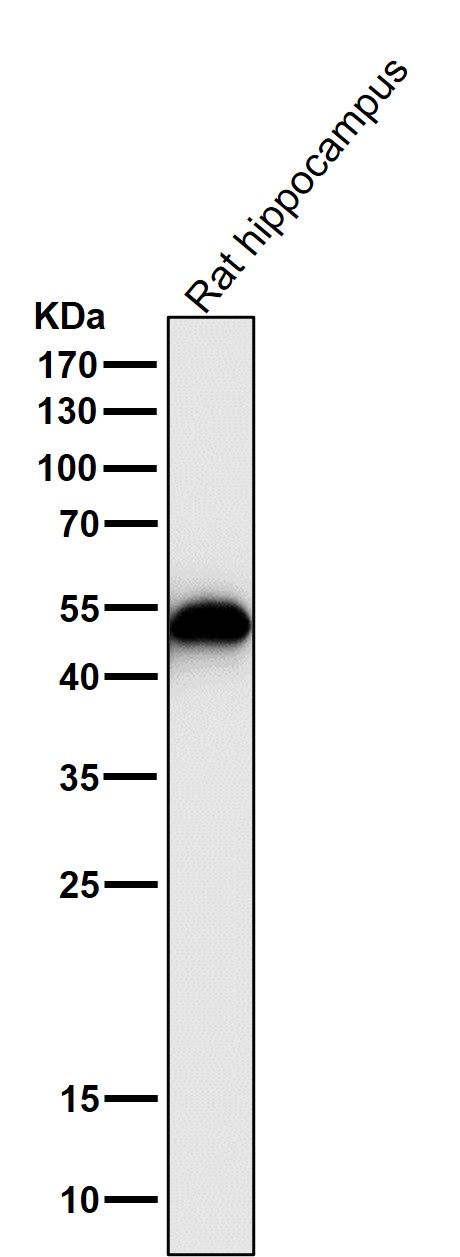
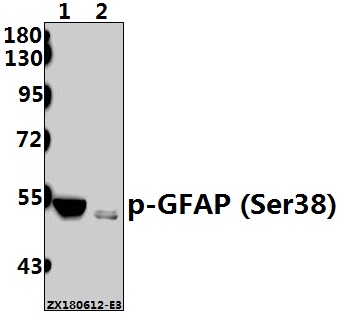
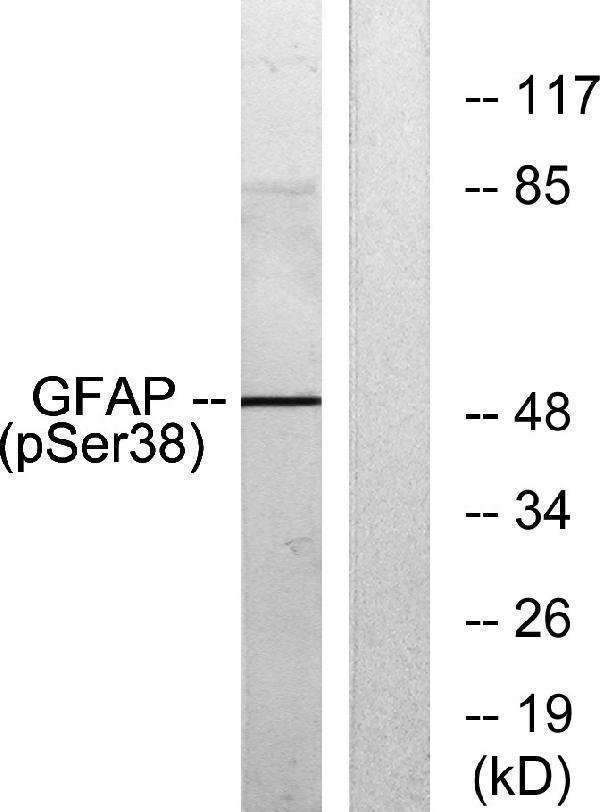
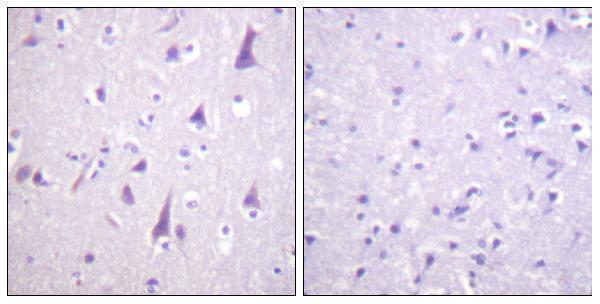
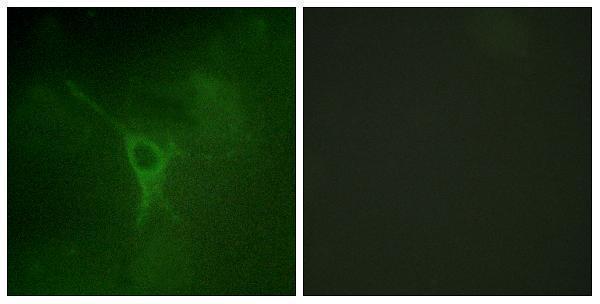
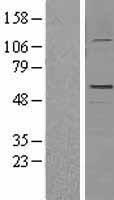
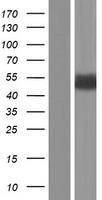
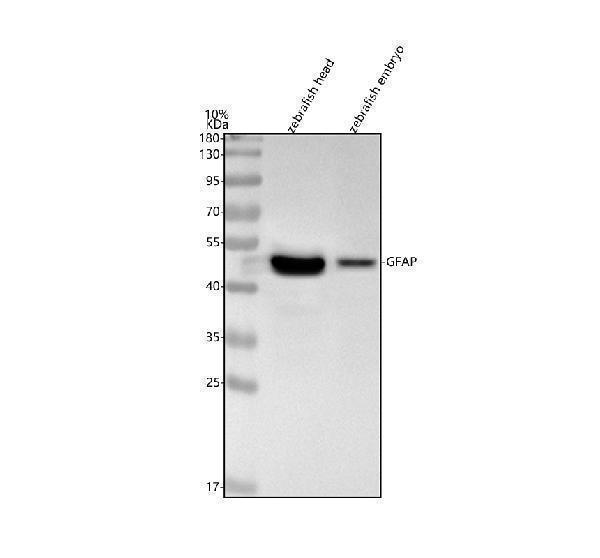
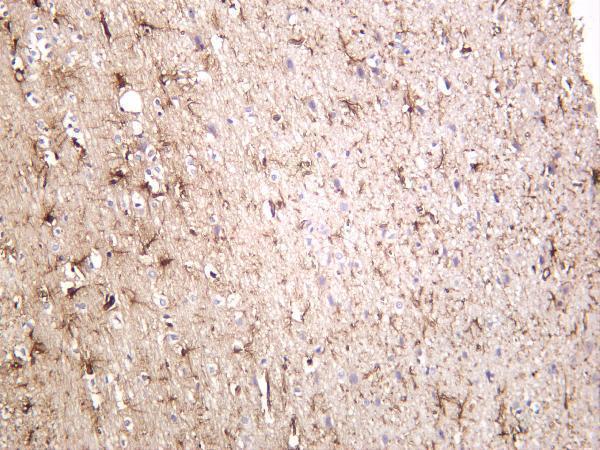
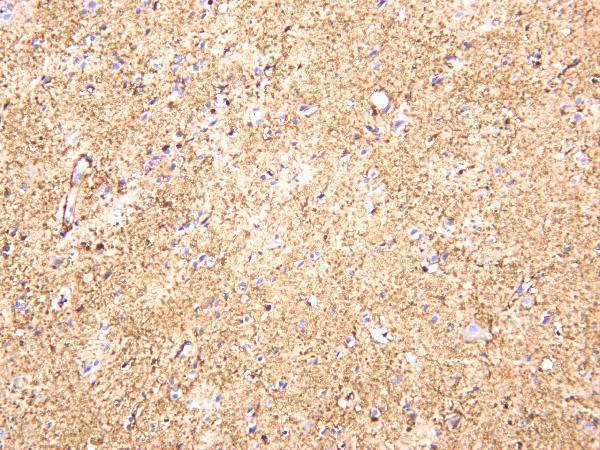
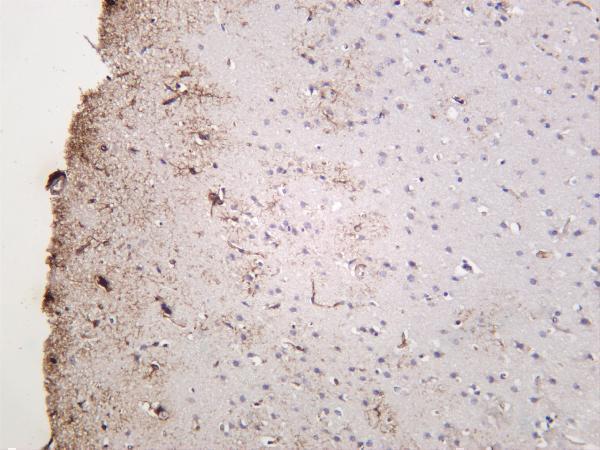
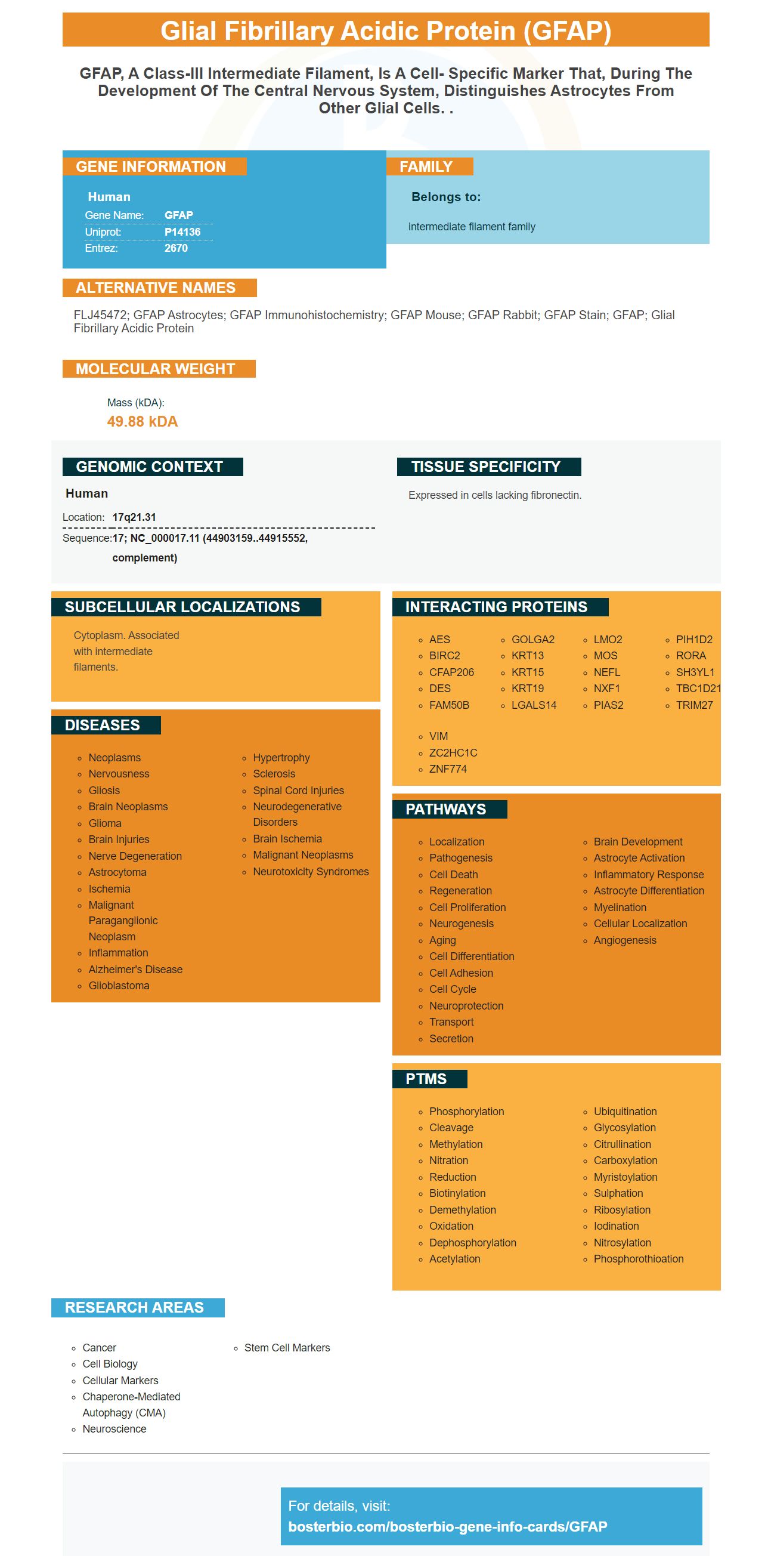
Facts about Glial fibrillary acidic protein.

| Human | |
|---|---|
| Gene Name: | GFAP |
| Uniprot: | P14136 |
| Entrez: | 2670 |

| Belongs to: |
|---|
| intermediate filament family |

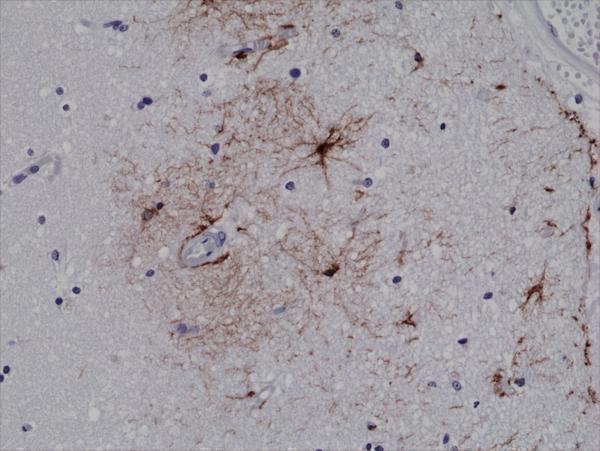
FLJ45472; GFAP astrocytes; GFAP immunohistochemistry; GFAP mouse; GFAP rabbit; GFAP stain; GFAP; glial fibrillary acidic protein
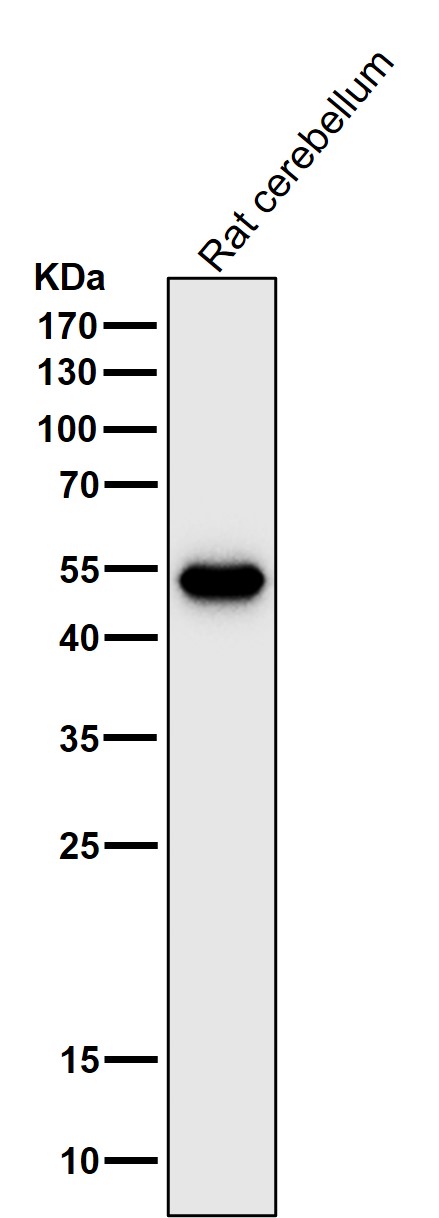
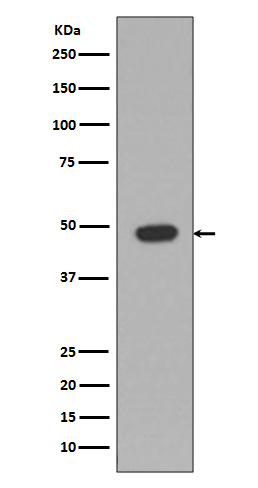
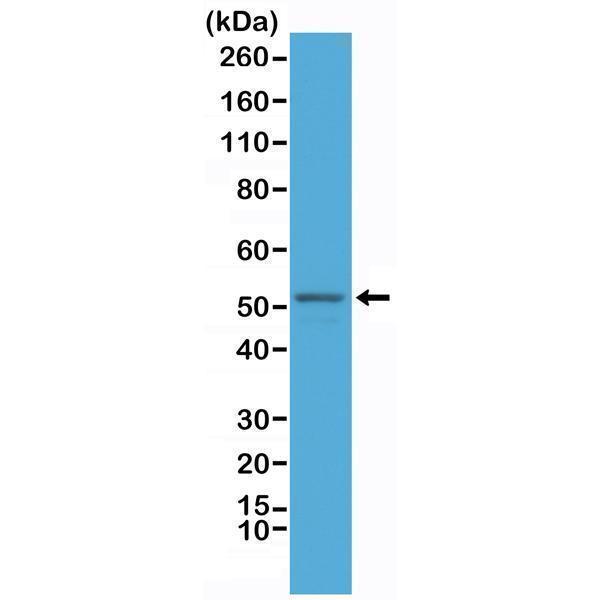
Mass (kDA):
49.88 kDA

| Human | |
|---|---|
| Location: | 17q21.31 |
| Sequence: | 17; NC_000017.11 (44903159..44915552, complement) |
Expressed in cells lacking fibronectin.
Cytoplasm. Associated with intermediate filaments.




PMID: 2740350 by Reeves S.A., et al. Molecular cloning and primary structure of human glial fibrillary acidic protein.
PMID: 2163003 by Brenner M., et al. Characterization of human cDNA and genomic clones for glial fibrillary acidic protein.
*Showing only the more recent 20. More publications can be found for each product on its corresponding product page