This website uses cookies to ensure you get the best experience on our website.
- Table of Contents

1 Citations 7 Q&As

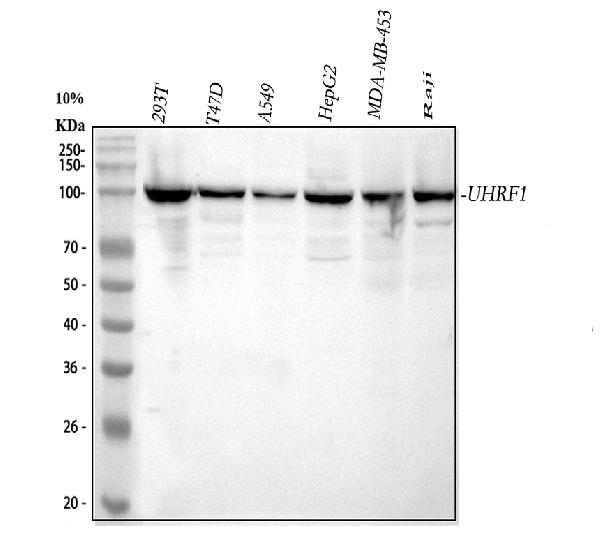
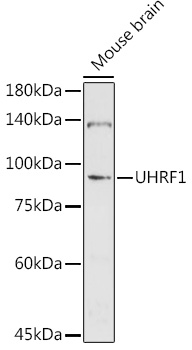
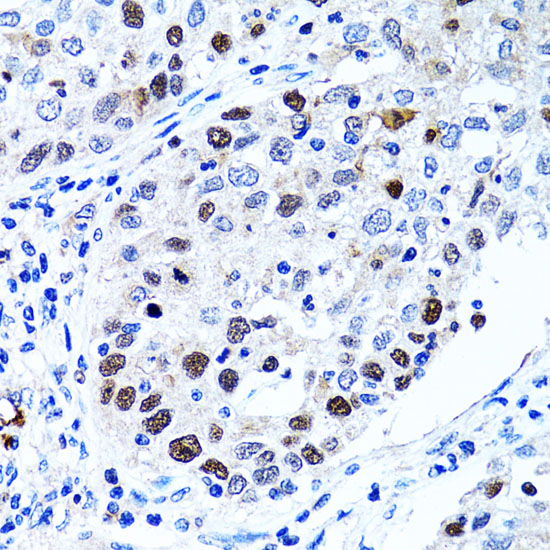
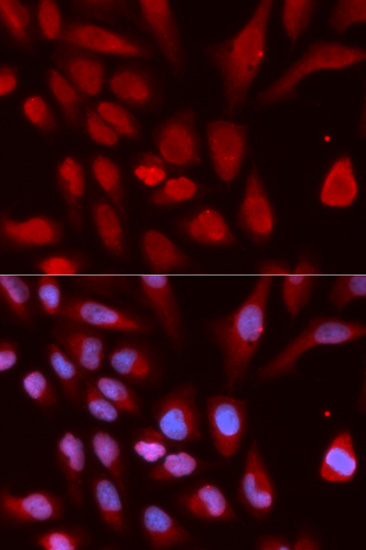
Facts about E3 ubiquitin-protein ligase UHRF1.
In addition to its role in maintenance of DNA methylation, also plays an integral role in chromatin modification: through its tudor-like regions and PHD- type zinc fingers, specifically recognizes and binds histone H3 trimethylated in'Lys-9' (H3K9me3) and unmethylated in'Arg-2' (H3R2me0), respectively, and recruits chromatin proteins. Enriched in pericentric heterochromatin where it recruits different chromatin modifiers required for this chromatin replication.
| Mouse | |
|---|---|
| Gene Name: | Uhrf1 |
| Uniprot: | Q8VDF2 |
| Entrez: | 18140 |

| Belongs to: |
|---|
| No superfamily |

E3 ubiquitin-protein ligase UHRF1; EC 6.3.2; EC 6.3.2.-; FLJ21925; hNP95; huNp95; ICBP90NP95; Inverted CCAAT box-binding protein of 90 kDa; Np95; Nuclear protein 95; Nuclear zinc finger protein Np95; RING finger protein 106; RNF106MGC138707; Transcription factor ICBP90; Ubiquitin-like PHD and RING finger domain-containing protein 1; ubiquitin-like with PHD and ring finger domains 1; ubiquitin-like, containing PHD and RING finger domains, 1; Ubiquitin-like-containing PHD and RING finger domains protein 1
Mass (kDA):
88.304 kDA

| Mouse | |
|---|---|
| Location: | 17|17 D |
| Sequence: | 17; |
Expressed in thymus, testis, spleen and lung. Within testis, expressed in almost all cells except elongated spermatids.


PMID: 9880673 by Fujimori A., et al. Cloning and mapping of Np95 gene which encodes a novel nuclear protein associated with cell proliferation.
PMID: 12084726 by Muto M., et al. Targeted disruption of Np95 gene renders murine embryonic stem cells hypersensitive to DNA damaging agents and DNA replication blocks.
*More publications can be found for each product on its corresponding product page