This website uses cookies to ensure you get the best experience on our website.
- Table of Contents

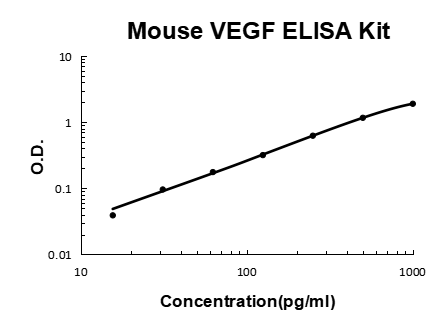
A comprehensive evaluation of Vascular Endothelial Growth Factor A (VEGFA) and VEGFR2 as prognostic biomarkers in bladder cancer, covering testing protocols and clinical integration strategies.
Vascular endothelial growth factor A (VEGFA) is a key driver of tumor angiogenesis and has emerged as a clinically significant biomarker for stratifying patient prognosis and guiding therapeutic decisions in bladder cancer.
Bladder cancer is among the most prevalent urological malignancies worldwide, with urothelial carcinoma accounting for the majority of cases. The ability to accurately predict disease progression and patient outcomes remains a central challenge in urological oncology. VEGFA, a potent pro-angiogenic cytokine, has attracted significant research interest as a tissue-based prognostic biomarker due to its central role in regulating tumor blood vessel formation.
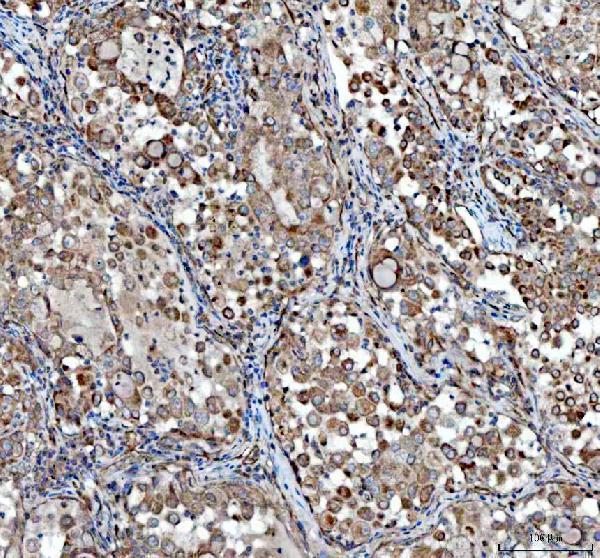
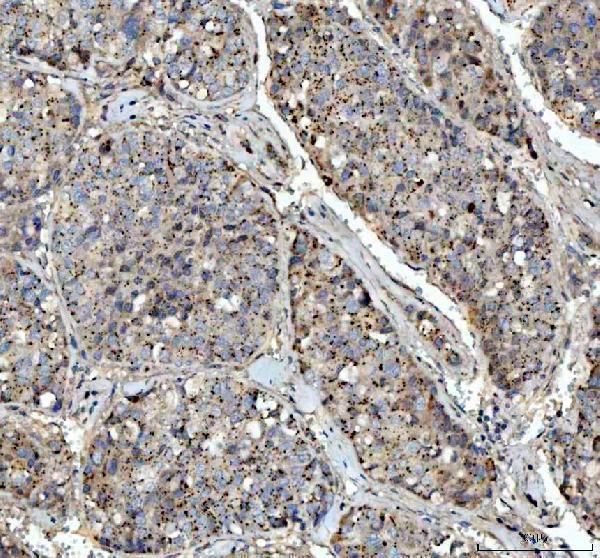
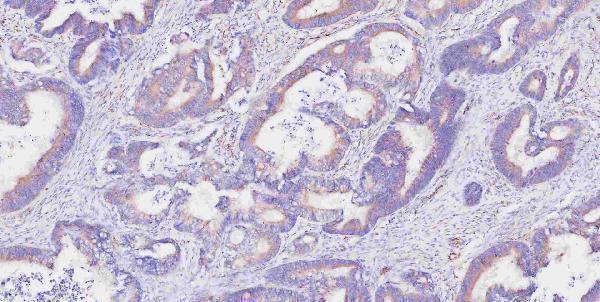
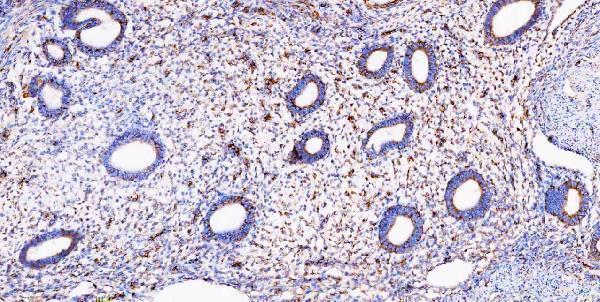
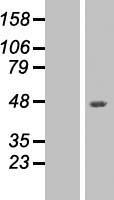
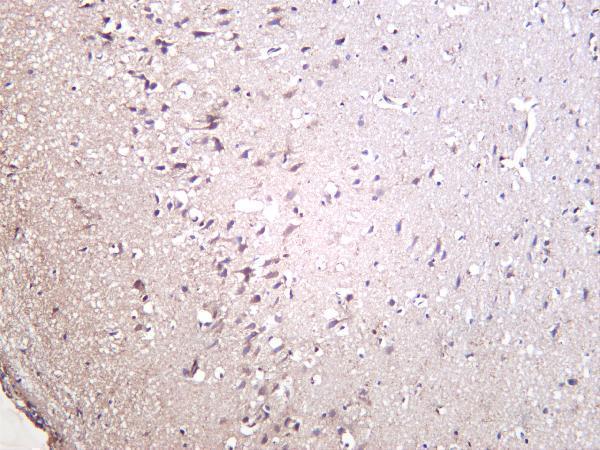
Elevated VEGFA expression in tumor tissue, as detected by immunohistochemistry (IHC), has been consistently associated with higher tumor grade, advanced pathological stage, lymphovascular invasion, and diminished overall survival in bladder cancer cohorts. Studies have demonstrated that patients with high VEGFA expression exhibit significantly shorter disease-free survival intervals compared to those with low or negative expression, underscoring the protein's utility as an independent prognostic indicator.
Beyond tissue-based IHC, serum and urine VEGFA concentrations have also been investigated as non-invasive prognostic indicators. Elevated circulating VEGFA levels have been linked to more aggressive disease phenotypes and poorer therapeutic responses, positioning VEGFA as a candidate biomarker across multiple biological compartments. The consistency of these findings across diverse patient populations strengthens the argument for its clinical adoption.
| VEGFA Expression Level | Tumor Stage Association | Prognostic Implication |
|---|---|---|
| Low / Negative | Superficial (Ta, T1) | Favorable overall survival |
| Moderate | Muscle-invasive (T2) | Intermediate prognosis |
| High / Overexpressed | Advanced (T3-T4, N+, M+) | Poor prognosis, high recurrence risk |
Critically, the prognostic value of VEGFA appears to extend beyond simple staging. In multivariate analyses controlling for established clinicopathological variables such as age, tumor size, and lymph node status, VEGFA expression has retained independent prognostic significance. This highlights its potential to refine risk stratification beyond what conventional staging systems alone can provide.
Evidence from clinical studies highlights several consistent findings regarding VEGFA expression patterns in bladder cancer.
VEGFA drives tumor angiogenesis by binding to endothelial receptors, stimulating new blood vessel formation that supplies oxygen and nutrients to the growing tumor mass, enabling invasion and metastasis.
Multivariate studies confirm VEGFA expression retains independent prognostic significance even after controlling for stage, grade, and lymph node status, providing additional risk stratification beyond standard clinicopathological parameters.
As a measurable biomarker and therapeutic target, VEGFA expression data can guide the selection of anti-angiogenic agents such as bevacizumab and sunitinib, aligning treatment choice with the molecular profile of the individual tumor.
While VEGFA represents the ligand in the VEGF signaling axis, its biological effects are primarily mediated through binding to Vascular Endothelial Growth Factor Receptor 2 (VEGFR2, also known as KDR/Flk-1). Assessing VEGFR2 expression in bladder tumor tissue provides a complementary and mechanistically relevant layer of prognostic information beyond VEGFA expression alone.
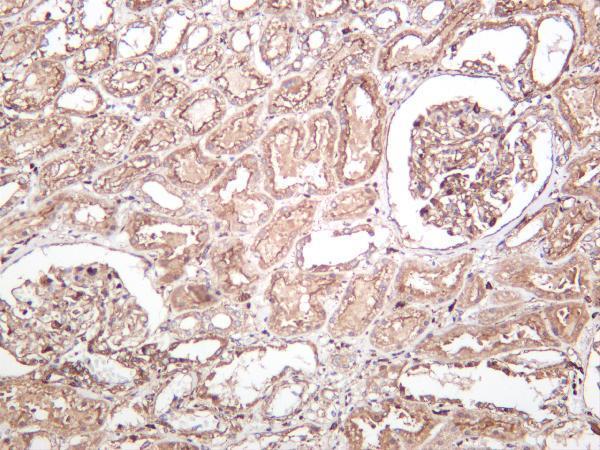
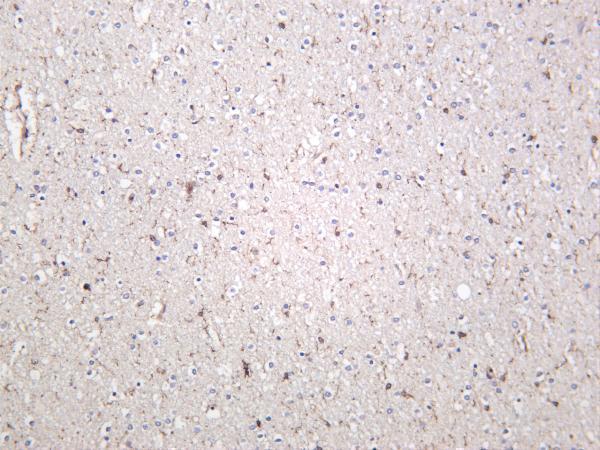
VEGFR2 is expressed not only on tumor-associated endothelial cells but has also been detected on bladder carcinoma cells themselves, indicating potential autocrine signaling loops that may confer additional growth advantages. Overexpression of VEGFR2 in tumor specimens has been correlated with enhanced microvessel density (MVD), a histological surrogate of angiogenic activity, and has been associated with shorter recurrence-free survival in bladder cancer patients.
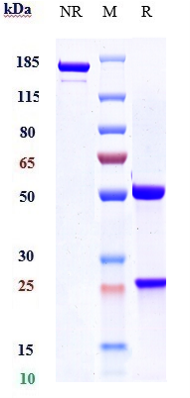
IHC-based VEGFR2 analysis on formalin-fixed paraffin-embedded (FFPE) tissue sections is the most widely employed method for receptor quantification in clinical research settings. Standardized antibody panels targeting the extracellular and intracellular domains of VEGFR2 allow for reproducible semi-quantitative scoring. Phosphorylated VEGFR2 (pVEGFR2), which reflects active receptor signaling, has been identified as a particularly informative biomarker because it indicates not merely receptor presence but functional ligand-receptor engagement within the tumor microenvironment.
VEGFR2 expression is commonly scored using the H-score system, calculated as:
H-score = (% cells with weak staining x 1) + (% cells with moderate staining x 2) + (% cells with strong staining x 3)
Scores range from 0 to 300. A threshold of H-score greater than 100 is frequently used to classify tumors as VEGFR2-high in published bladder cancer cohorts, though cut-offs should be validated within each institutional dataset.
Expression of phosphorylated VEGFR2 (pVEGFR2 Y1175) correlates most closely with downstream ERK and AKT pathway activation and is the most functionally relevant readout for anti-angiogenic therapy selection.
Leveraging both VEGFA and VEGFR2 in concert, while anchoring findings within standardized protocols and individualized clinical data, maximizes the prognostic precision achievable in bladder cancer management.
Assessing VEGFA and VEGFR2 independently provides valuable prognostic information, but the greatest discriminatory power is achieved when both biomarkers are evaluated in combination. A co-expression analysis approach acknowledges that tumor aggressiveness is not solely a function of ligand overproduction or receptor overexpression, but rather the product of active ligand-receptor signaling within the tumor microenvironment.
Research on bladder cancer cohorts has demonstrated that patients with concurrent high VEGFA and high VEGFR2 expression exhibit the poorest prognosis across multiple endpoints including overall survival, progression-free survival, and recurrence-free survival. Conversely, tumors with low expression of both markers are associated with the most favorable outcomes. Intermediate groups, those with high expression of one marker but not the other, display prognoses that fall between these extremes, reinforcing the additive value of the dual assessment strategy.
From a mechanistic standpoint, the co-expression phenotype reflects a fully activated VEGF signaling axis: abundant ligand, engaged receptor, and downstream pathway activation driving tumor angiogenesis and potentially direct tumor cell growth. This phenotype is also most likely to respond to VEGF pathway-targeted therapies, making the combined biomarker profile directly actionable from a therapeutic standpoint.
| VEGFA Status | VEGFR2 Status | Prognostic Category | Clinical Implication |
|---|---|---|---|
| High | High | Worst prognosis group | Anti-angiogenic therapy candidate; intensive follow-up |
| High | Low | Intermediate prognosis | Evaluate alternative pathway activation |
| Low | High | Intermediate prognosis | Monitor receptor expression dynamics |
| Low | Low | Favorable prognosis group | Standard surveillance; lower recurrence risk |
Statistically, combined biomarker models show improved C-statistics (a measure of discrimination) compared to models incorporating either marker alone or conventional staging variables in isolation. The incorporation of VEGFA and VEGFR2 co-expression into nomogram-based prognostic tools represents a practical pathway toward clinical translation of this dual biomarker approach.
Reliable prognostic biomarker data requires rigorous, reproducible analytical protocols. The following steps outline the key stages of a standardized VEGFA and VEGFR2 testing workflow for bladder cancer tissue specimens.
Biomarker data, however informative in isolation, reaches its greatest clinical utility when systematically integrated with the full landscape of a patient's clinical profile. For bladder cancer patients, this includes pathological staging and grading, surgical margin status, lymphovascular invasion, lymph node involvement, performance status, comorbidity burden, prior treatment history, and patient preferences regarding treatment intensity.
A structured biomarker-clinical integration workflow begins with molecular profiling of the tumor specimen at the time of definitive surgical intervention or initial diagnostic workup. VEGFA and VEGFR2 expression scores are entered alongside conventional staging data into a unified patient record or multidisciplinary tumor board database. Prognostic nomograms that incorporate both molecular and clinical variables can then generate individualized risk estimates that inform surveillance intensity, adjuvant treatment decisions, and candidacy for clinical trials targeting the VEGF pathway.
In practice, patients identified as high-risk based on combined high VEGFA/VEGFR2 expression may be prioritized for early initiation of adjuvant systemic therapy, more frequent cystoscopic surveillance, or enrolment in trials evaluating VEGF-targeted regimens such as ramucirumab or cabozantinib. Low-risk molecular profiles may support de-escalation strategies that reduce treatment burden and associated toxicity without compromising oncological outcomes.
| Clinical Variable | Relevance to VEGFA/VEGFR2 Context |
|---|---|
| Pathological Stage (T category) | Higher T stage correlates with elevated VEGFA expression frequency |
| Tumor Grade | High-grade tumors show significantly greater VEGFR2 overexpression rates |
| Lymphovascular Invasion (LVI) | LVI presence amplifies prognostic impact of high dual biomarker status |
| Nodal Status (N category) | Node-positive disease combined with high VEGFA defines the highest-risk subgroup |
| Prior Intravesical Therapy | BCG-refractory status may correlate with upregulated VEGF signaling |
Common questions regarding the clinical and research application of VEGFA and VEGFR2 biomarkers in bladder cancer.
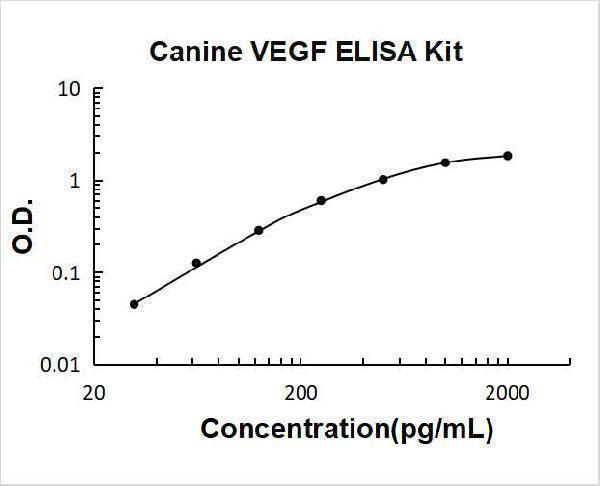
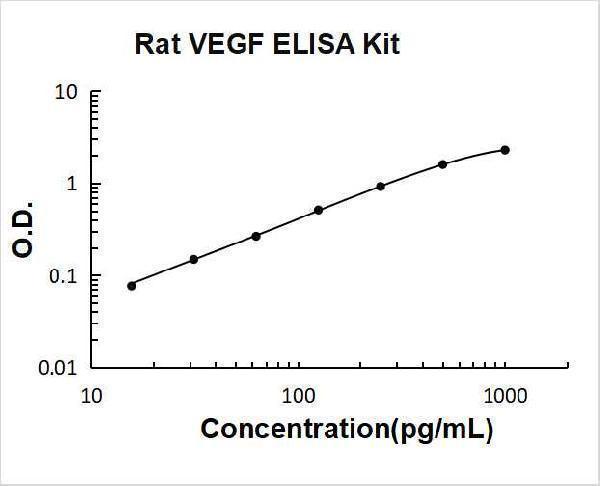
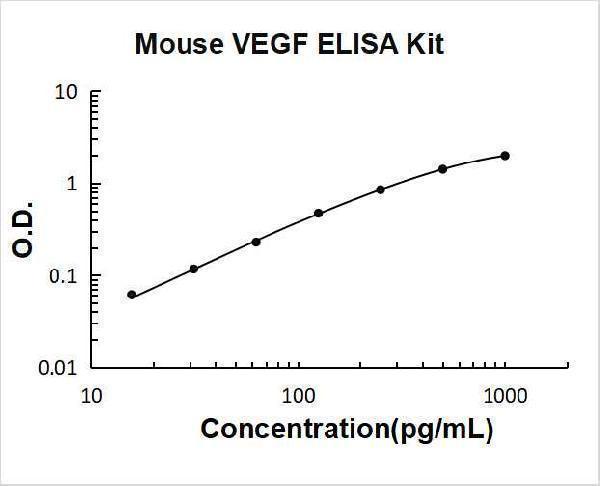
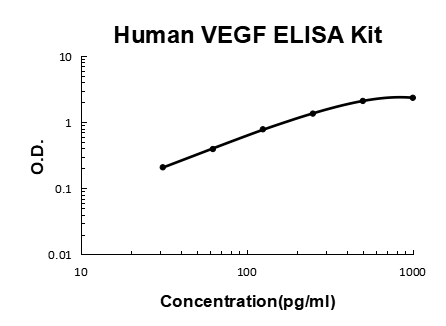
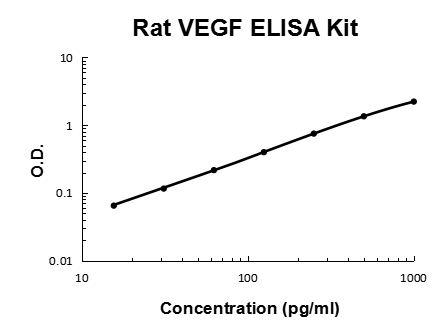
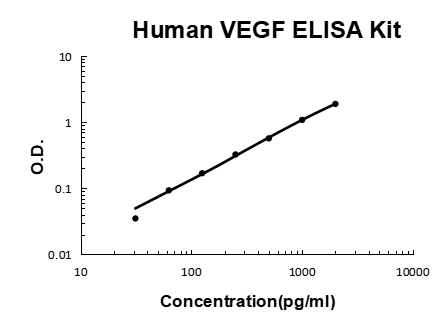
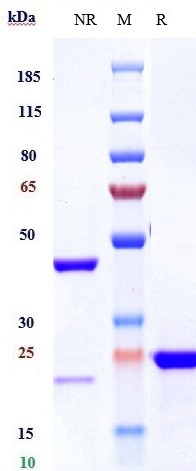
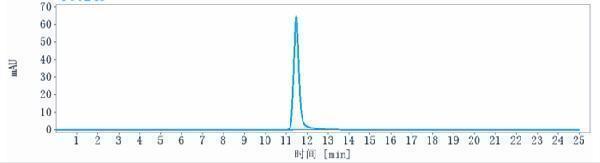
Access validated antibodies, ELISA kits, and IHC reagents for VEGFA and VEGFR2 research in bladder cancer and other oncology applications.
195 Citations 20 Q&As

83 Citations 18 Q&As
75 Citations 4 Q&As
191 Citations 18 Q&As
51 Citations 5 Q&As
17 Citations 17 Q&As
4 Citations 16 Q&As

5 Citations

18 Citations
9 Citations






Facts about Vascular endothelial growth factor A.

Binds to the FLT1/VEGFR1 and KDR/VEGFR2 receptors, heparan sulfate and heparin. NRP1/Neuropilin-1 binds isoforms VEGF-165 and VEGF-145.
| Human | |
|---|---|
| Gene Name: | VEGFA |
| Uniprot: | P15692 |
| Entrez: | 7422 |

| Belongs to: |
|---|
| PDGF/VEGF growth factor family |

MVCD1; VAS; vascular endothelial growth factor A; Vascular permeability factor; Vasculotropin; VEGF; VEGFA; VEGF-A; VEGFMGC70609; VPF; VPFvascular endothelial growth factor
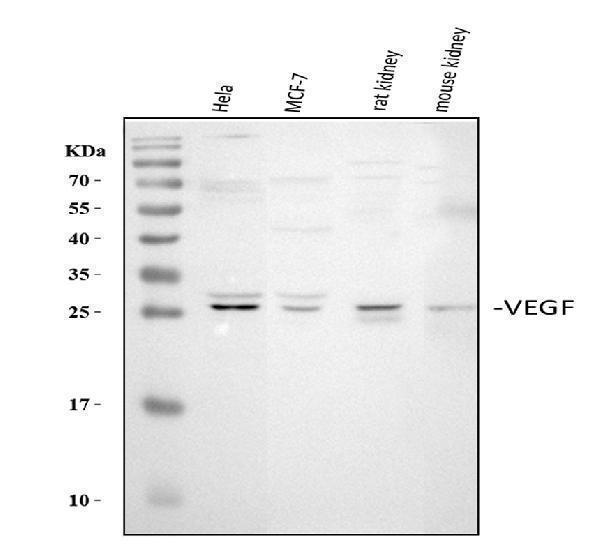
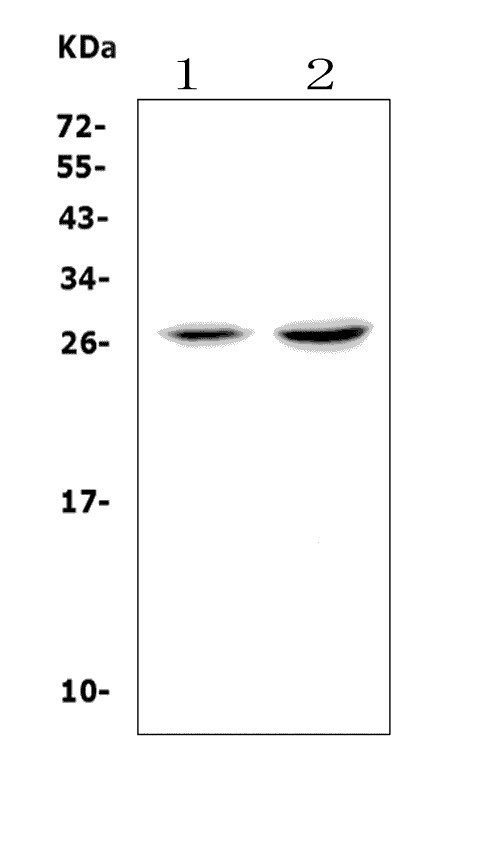
Mass (kDA):
27.042 kDA

| Human | |
|---|---|
| Location: | 6p21.1 |
| Sequence: | 6; NC_000006.12 (43770209..43786487) |
Isoform VEGF189, isoform VEGF165 and isoform VEGF121 are widely expressed. Isoform VEGF206 and isoform VEGF145 are not widely expressed. A higher level expression seen in pituitary tumors as compared to the pituitary gland.
Secreted. VEGF121 is acidic and freely secreted. VEGF165 is more basic, has heparin-binding properties and, although a significant proportion remains cell-associated, most is freely secreted. VEGF189 is very basic, it is cell-associated after secretion and is bound avidly by heparin and the extracellular matrix, although it may be released as a soluble form by heparin, heparinase or plasmin.




PMID: 2479986 by Leung D.W., et al. Vascular endothelial growth factor is a secreted angiogenic mitogen.
PMID: 2479987 by Keck P.J., et al. Vascular permeability factor, an endothelial cell mitogen related to PDGF.
*Showing only the more recent 20. More publications can be found for each product on its corresponding product page