This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
A comprehensive clinical reference covering EGFR biomarker testing, ALK inhibitor therapy, MET amplification, KRAS mutation analysis, pre-validated protocols, and pemetrexed efficacy in non-small-cell lung cancer.
The landscape of non-small-cell lung cancer (NSCLC) treatment has been transformed over the past two decades by the identification and clinical application of actionable molecular biomarkers. Chief among these is the epidermal growth factor receptor (EGFR), whose activating mutations predict sensitivity to targeted tyrosine kinase inhibitors (TKIs). Alongside EGFR, markers including ALK rearrangements, MET amplifications, and KRAS mutations collectively guide treatment stratification, enabling clinicians to select or exclude specific therapeutic agents with a precision that was impossible under purely histological classification.
This article consolidates current egfr biomarker knowledge across six clinical domains: integrating EGFR mutation testing into routine NSCLC workup, leveraging ALK inhibitor crizotinib for advanced disease, addressing acquired resistance through MET amplification detection, applying KRAS analysis for therapy exclusion, implementing pre-validated testing protocols to shorten turnaround times, and reviewing the clinical evidence base for pemetrexed in lung cancer trials.
Integrating EGFR biomarker analysis as a standard diagnostic step in non-small-cell lung cancer treatment planning.
EGFR mutations are detected in approximately 10-15% of Western NSCLC patients and up to 50% of Asian patients with adenocarcinoma histology. The most common activating mutations are exon 19 deletions and the L858R point mutation in exon 21, together accounting for roughly 85-90% of all sensitizing EGFR alterations. Patients harbouring these mutations derive substantial clinical benefit from first-, second-, and third-generation EGFR TKIs, including erlotinib, afatinib, and osimertinib.
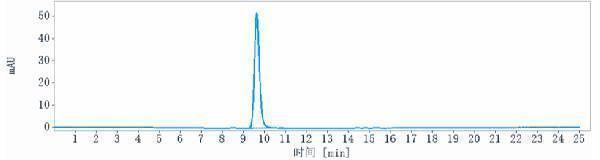
Current guidelines from major oncology bodies recommend reflex EGFR mutation testing at diagnosis for all patients with advanced, non-squamous NSCLC, and selectively for mixed or unknown histology. Testing should be performed on tumour tissue whenever possible, with plasma-based liquid biopsy serving as a complementary option when tissue is insufficient or unavailable. Real-time PCR platforms, next-generation sequencing (NGS) panels, and allele-specific PCR are the principal methodologies deployed in certified molecular pathology laboratories.
| Mutation | Exon | Frequency | TKI Sensitivity |
|---|---|---|---|
| Exon 19 Deletion | 19 | ~45% | High (1st, 2nd, 3rd gen) |
| L858R Point Mutation | 21 | ~40% | High (1st, 2nd, 3rd gen) |
| G719X | 18 | ~3% | Moderate (afatinib) |
| Exon 20 Insertion | 20 | ~5-10% | Low (standard TKIs) |
| T790M (acquired) | 20 | ~50% post-progression | High (osimertinib) |
The detection of T790M in plasma following progression on first- or second-generation TKI therapy has become a pivotal indication for switching to osimertinib. Liquid biopsy in this context shortens the time from clinical progression to therapeutic decision, avoiding invasive re-biopsy procedures and preserving patient quality of life during a critical transition.
How the first ALK inhibitor transformed outcomes for a molecularly defined NSCLC subpopulation.
Anaplastic lymphoma kinase (ALK) gene rearrangements, most commonly the EML4-ALK fusion, occur in approximately 3-5% of NSCLC cases. These rearrangements define a distinct molecular subtype enriched in younger patients, never or light smokers, and adenocarcinoma histology. The identification of ALK rearrangement as a driver alteration led directly to the development of crizotinib, a first-in-class oral ALK/MET/ROS1 inhibitor approved for ALK-positive advanced NSCLC based on landmark phase III clinical evidence.
The PROFILE 1014 trial demonstrated that crizotinib significantly improved progression-free survival (PFS) compared to platinum-based chemotherapy in previously untreated ALK-positive advanced NSCLC (10.9 months vs. 7.0 months, HR 0.45). Overall response rate with crizotinib reached 74% versus 45% in the chemotherapy arm. These results established crizotinib as the standard first-line therapy for ALK-rearranged NSCLC and validated ALK as a central EGFR biomarker-class target alongside EGFR itself.
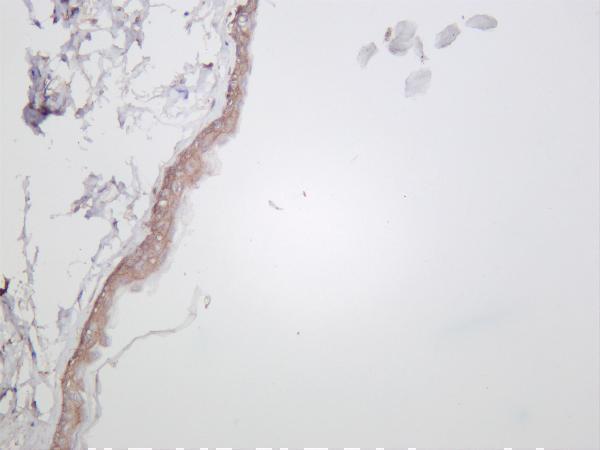
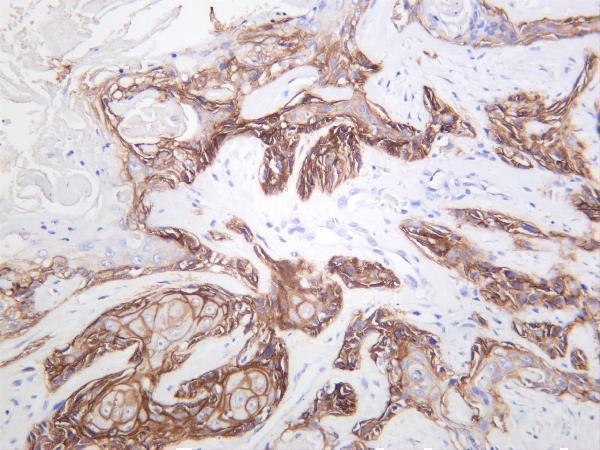
Fluorescence in situ hybridisation (FISH) remains the FDA-approved companion diagnostic for ALK-positive NSCLC, though immunohistochemistry (IHC) with D5F3 clone and NGS panels are increasingly accepted in clinical practice for their speed, throughput, and capacity to simultaneously screen multiple biomarkers. Co-testing for EGFR biomarker status and ALK in a multiplex panel is now recommended to streamline the diagnostic pathway for newly diagnosed advanced NSCLC patients.
FDA-approved companion diagnostic for ALK-positive NSCLC. Detects chromosomal rearrangements with high specificity using fluorescent probes targeting ALK break-apart regions.
Rapid, cost-effective alternative for ALK detection on FFPE tissue. High sensitivity when performed with validated automated platforms such as the Ventana OptiView amplification system.
Simultaneous detection of ALK, EGFR, ROS1, MET, KRAS, and other actionable alterations in a single assay. Preferred when tissue is limited and comprehensive biomarker profiling is required.
Overcoming acquired resistance in EGFR-mutant NSCLC through MET pathway characterisation.
Acquired resistance to EGFR TKI therapy is an inevitable clinical challenge. While T790M gatekeeper mutation accounts for approximately 50-60% of resistance to first- and second-generation TKIs, MET proto-oncogene amplification emerges as a resistance mechanism in 5-20% of cases, including as a co-occurring resistance event alongside T790M and as the predominant mechanism of resistance to osimertinib. MET amplification activates the PI3K/AKT and RAS/MAPK downstream signalling cascades independently of EGFR, effectively bypassing TKI blockade.
Identifying MET amplification at progression is therefore clinically actionable. Combinations of EGFR TKIs with MET inhibitors such as savolitinib, capmatinib, and tepotinib are under active clinical investigation and have shown promising activity in MET-amplified, EGFR-mutant post-progression cohorts. The SAVANNAH and GEOMETRY mono-1 trials exemplify this therapeutic strategy, with response rates in the 30-65% range depending on the degree of MET amplification (gene copy number or FISH-based MET-to-CEP7 ratio).
| Method | Platform | Clinical Utility |
|---|---|---|
| FISH (MET/CEP7 ratio) | Tissue | Gold standard; stratifies high vs. low amplification |
| NGS (copy number variation) | Tissue / ctDNA | Comprehensive; concurrent biomarker profiling |
| IHC (MET protein expression) | FFPE tissue | Rapid screen; correlates imperfectly with amplification |
| RT-PCR (MET exon 14 skipping) | RNA-based | Detects splice-site mutations causing MET activation |
For optimal clinical decision-making, MET testing at progression should be incorporated into a comprehensive re-biopsy or liquid biopsy panel that simultaneously evaluates T790M status, MET amplification, EGFR amplification, and other emergent resistance alterations. This multi-biomarker approach at progression mirrors the expanded egfr biomarker profiling performed at initial diagnosis and ensures that therapeutic options are not overlooked.
Using KRAS status as a negative predictive biomarker to guide and exclude specific treatment strategies.
KRAS mutations are the most common oncogenic driver in NSCLC, detected in approximately 25-30% of all lung adenocarcinomas, with KRAS G12C representing the most frequent single variant (approximately 13% of NSCLC overall). Historically, KRAS mutations have served primarily as a predictive biomarker for exclusion from anti-EGFR therapies in colorectal cancer and as a general negative prognostic indicator in lung cancer. In NSCLC, KRAS mutations and EGFR mutations are mutually exclusive at the clonal level in the vast majority of cases, making concurrent positivity a signal for scrutiny of the testing result rather than biological co-occurrence.
The mutual exclusivity of KRAS and EGFR mutations is clinically important because a patient harbouring a KRAS mutation is unlikely to benefit from EGFR TKI therapy. In clinical practice, KRAS mutation testing therefore serves as a rapid preliminary exclusion step: a positive KRAS result effectively removes EGFR-targeted therapy from the treatment algorithm, directs the clinician toward standard chemotherapy regimens or immunotherapy, and reserves EGFR testing resources for KRAS-negative cases when comprehensive NGS is not performed upfront.
The emergence of covalent KRAS G12C inhibitors, most notably sotorasib (AMG 510) and adagrasib (MRTX849), has fundamentally repositioned KRAS from an undruggable target to an actionable oncogene in its own right. The CodeBreaK 100 phase II trial demonstrated an objective response rate of 37.1% and a disease control rate of 80.8% with sotorasib in previously treated KRAS G12C-mutant NSCLC. KRAS G12C status is now a positive predictive biomarker in its own right, warranting reflex testing as part of a comprehensive lung cancer molecular panel. The broader KRAS mutation landscape (G12D, G12V, G13C) remains without approved targeted therapy, preserving the exclusion-focused role of non-G12C KRAS mutations for the time being.
| KRAS Variant | Frequency in NSCLC | Targeted Agent Available |
|---|---|---|
| G12C | ~13% | Sotorasib, Adagrasib |
| G12D | ~4% | None approved (trials ongoing) |
| G12V | ~5% | None approved |
| G13C | ~1% | None approved |
| Other KRAS | ~6% | None approved |
Implementing standardised, pre-validated workflows to accelerate EGFR biomarker reporting and inform timely clinical decisions.
Reviewing the evidence base for pemetrexed as a chemotherapy partner in NSCLC, particularly in the context of biomarker-informed patient selection.
Pemetrexed is a multitargeted antifolate that inhibits thymidylate synthase (TS), dihydrofolate reductase (DHFR), and glycinamide ribonucleotide formyltransferase (GARFT), disrupting folate metabolism and purine/pyrimidine synthesis. Its clinical efficacy in lung cancer is strongly associated with histological subtype, which serves as a surrogate biomarker for TS expression. Squamous cell carcinoma expresses significantly higher levels of TS compared to adenocarcinoma, conferring relative resistance to pemetrexed, while adenocarcinomas and large-cell carcinomas are more sensitive. This observation underpins current clinical practice guidelines that restrict pemetrexed use to non-squamous NSCLC.
The pivotal JMDB phase III trial (Scagliotti et al., 2008) established pemetrexed plus cisplatin as equivalent in overall survival to gemcitabine plus cisplatin across all NSCLC histologies, with a significant survival advantage for pemetrexed in non-squamous histology (OS: 12.6 vs. 10.9 months) and an inferior outcome in squamous histology (OS: 9.4 vs. 10.8 months). Subsequent studies extended pemetrexed into maintenance and combination settings, reinforcing its central role in non-squamous NSCLC management.
In the era of targeted therapy and immunotherapy, pemetrexed remains clinically relevant both as a chemotherapy backbone in combination with pembrolizumab (KEYNOTE-189 regimen) and as a component of chemotherapy-targeted therapy combinations under clinical investigation. For EGFR-mutant NSCLC patients who progress on TKI therapy and have exhausted targeted options, platinum-pemetrexed chemotherapy provides a well-tolerated and effective subsequent treatment choice, particularly in the context of EGFR biomarker-informed patient management where the therapeutic trajectory has been defined from the outset.
Common clinical and scientific questions about EGFR biomarker testing and related molecular markers in NSCLC.
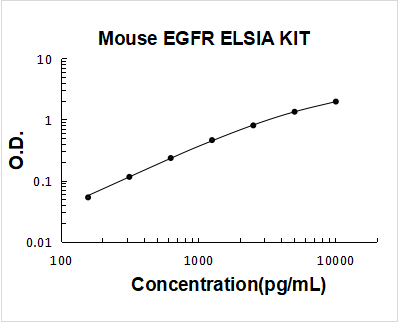
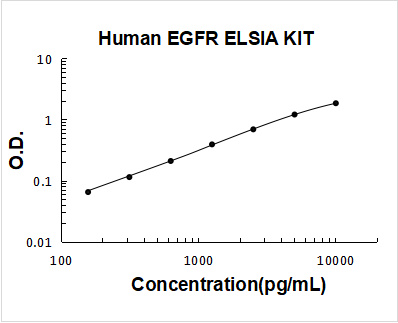
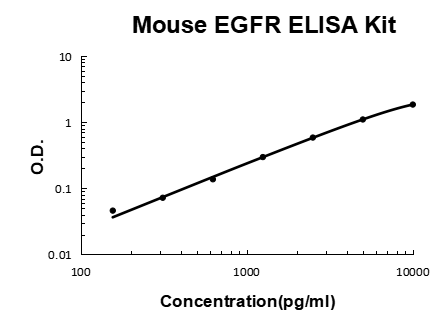
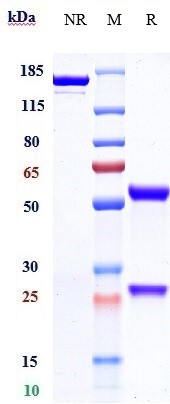
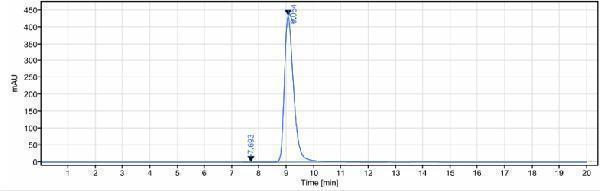
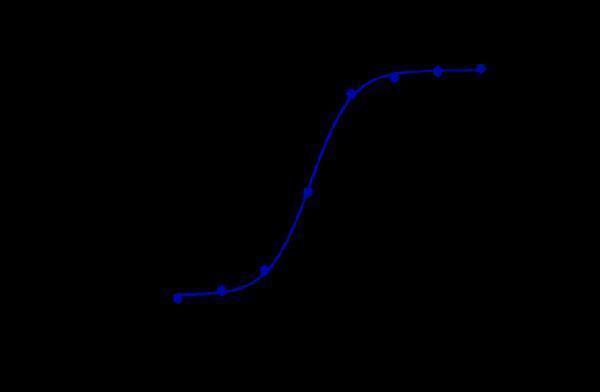
Explore validated antibodies, ELISA kits, and molecular reagents for EGFR, ALK, MET, and KRAS research. Contact our scientific support team for guidance on assay selection and protocol optimisation.
2 Citations 8 Q&As
5 Citations 8 Q&As
6 Citations











7 Citations
3 Citations
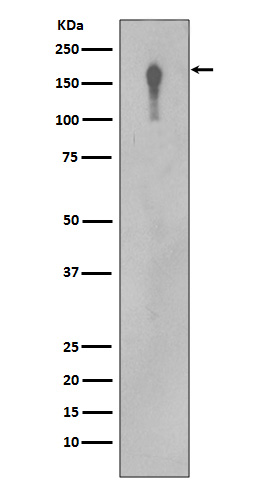
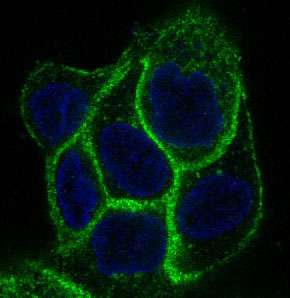
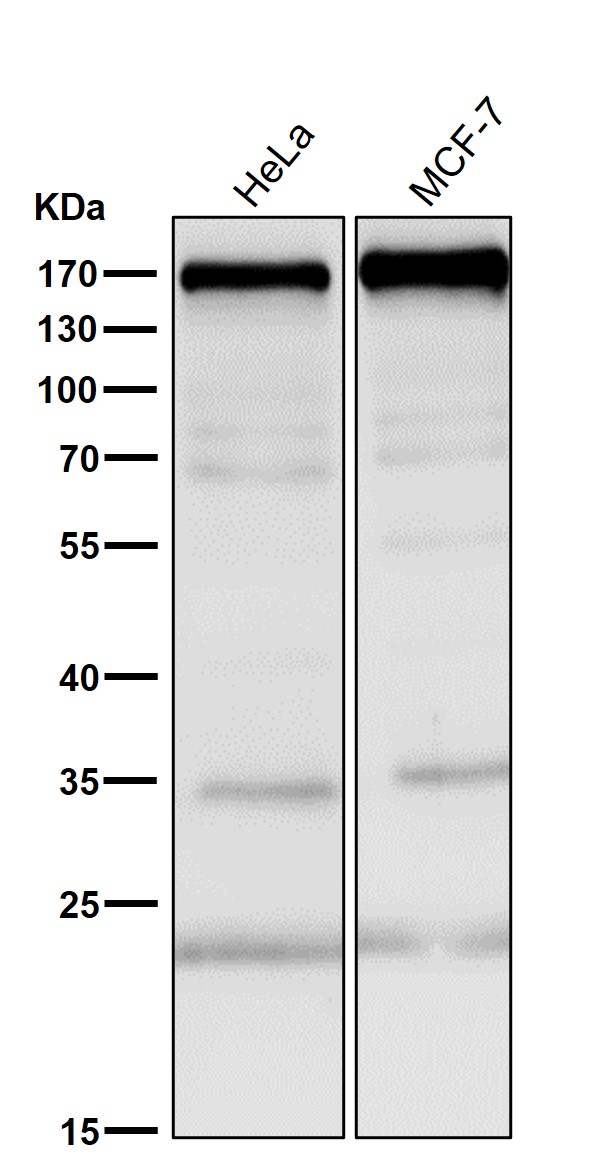
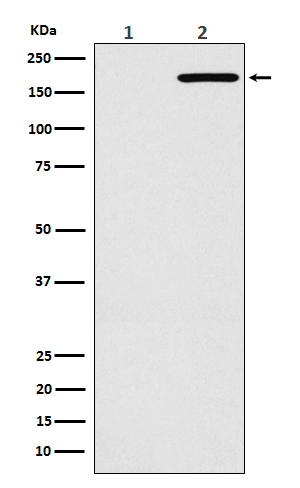

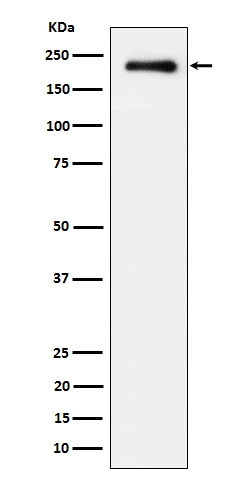

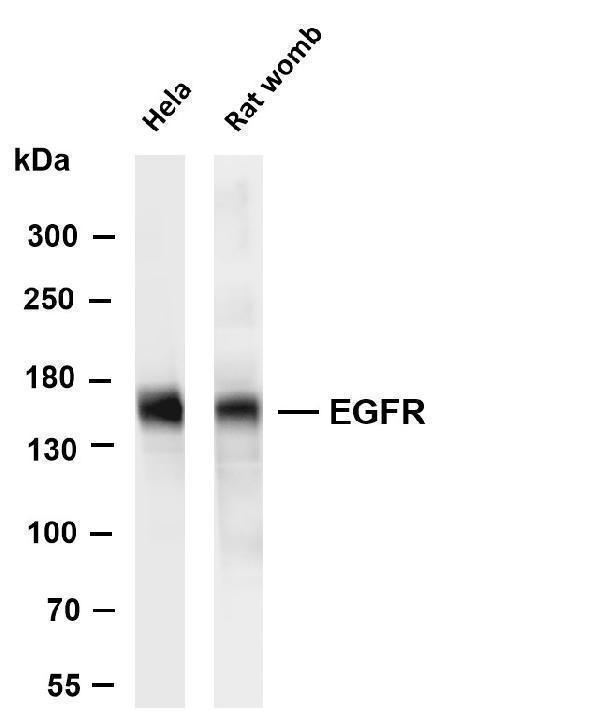
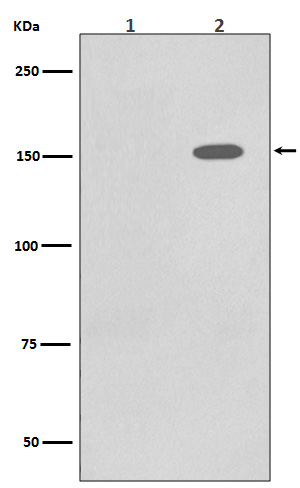
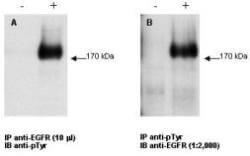
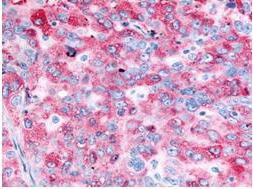
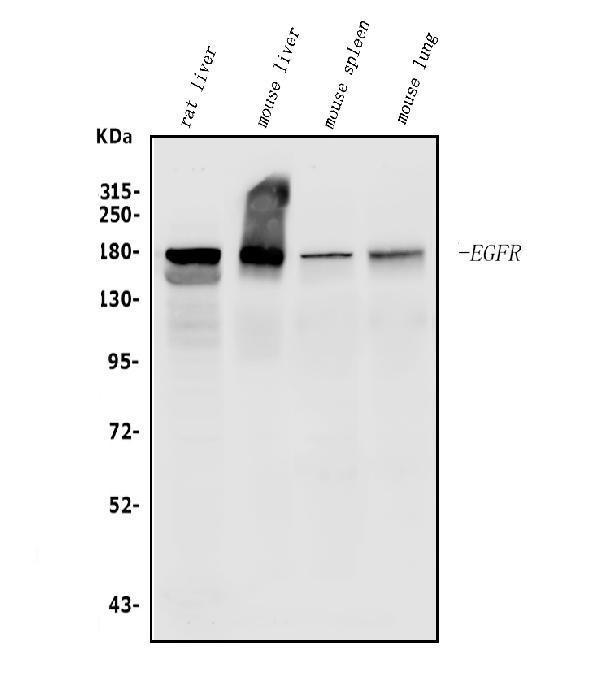
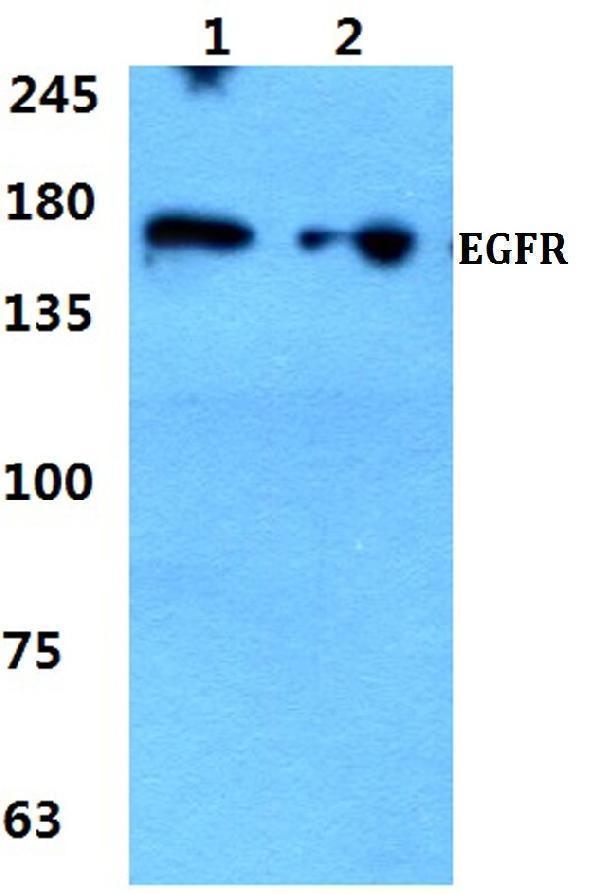
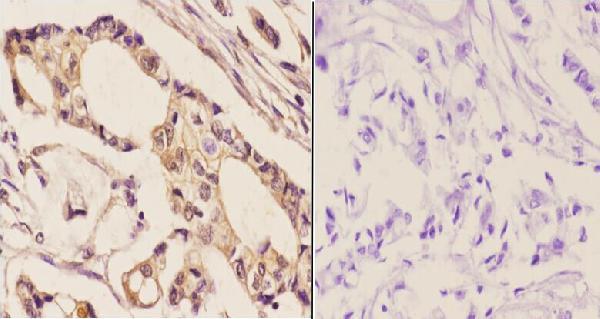
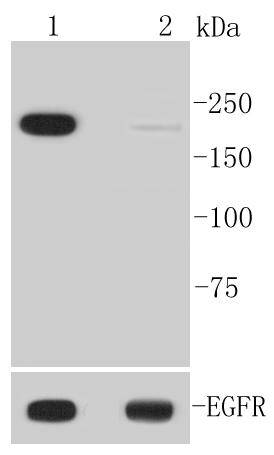
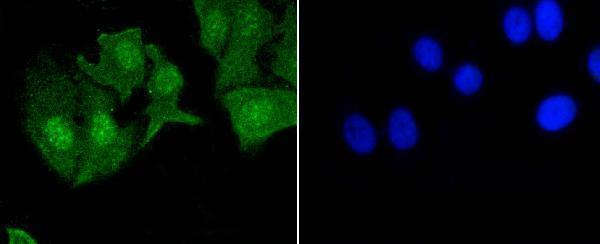
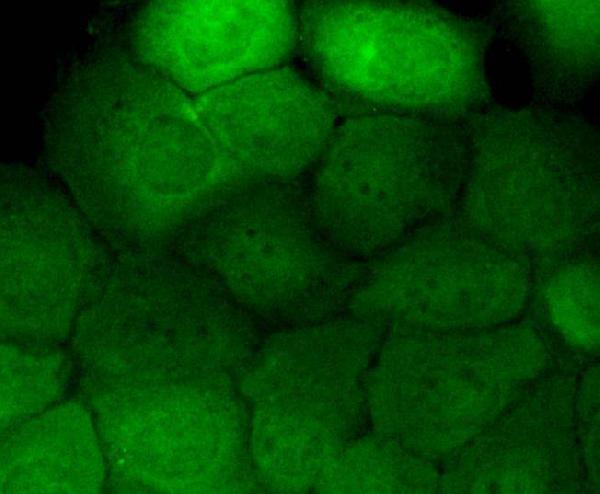
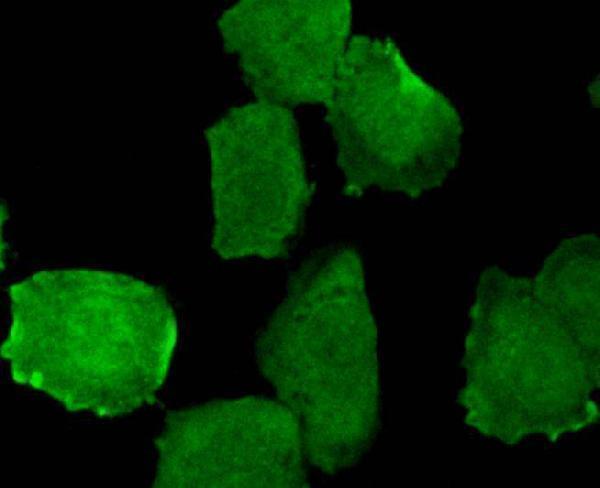
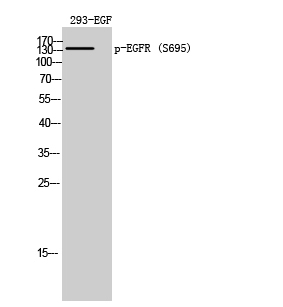
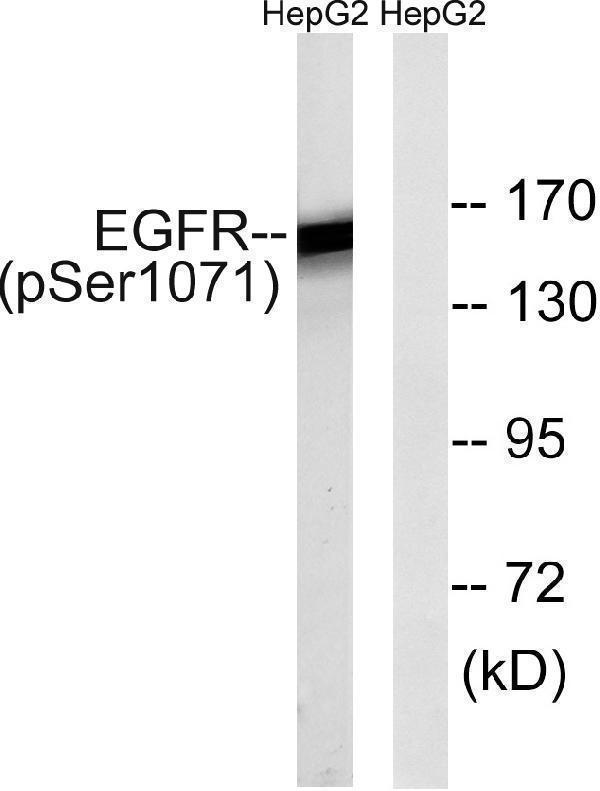
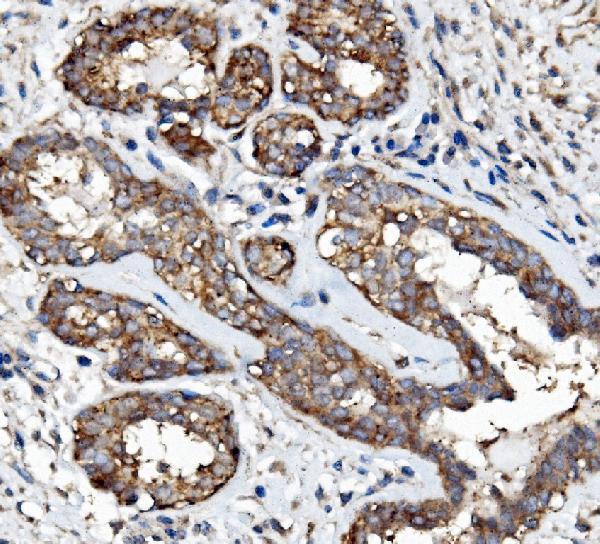
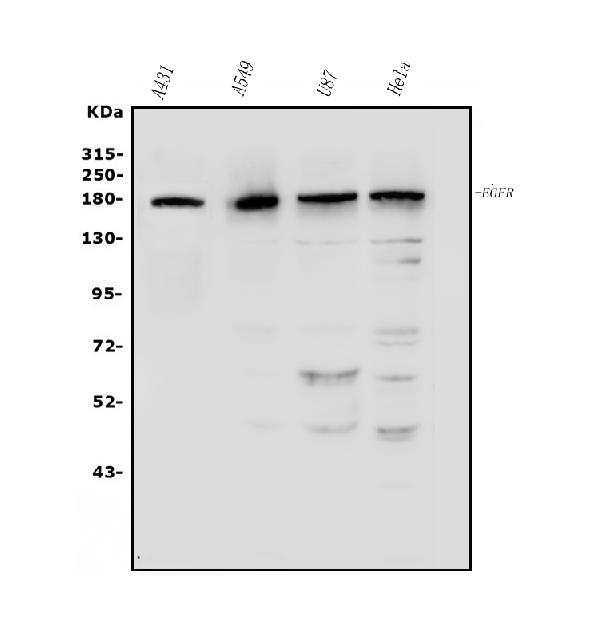
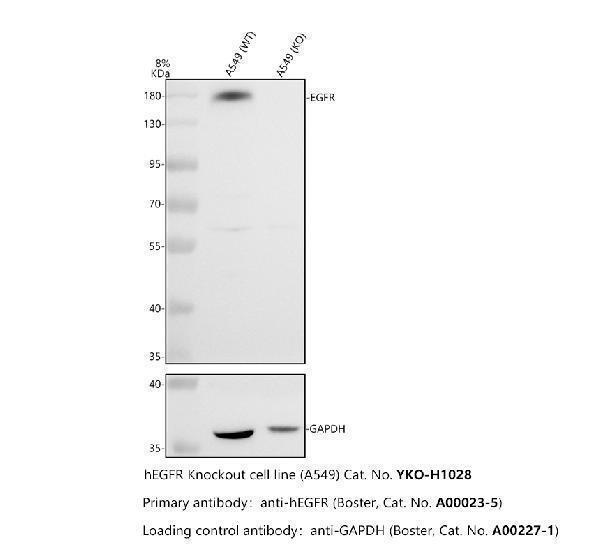
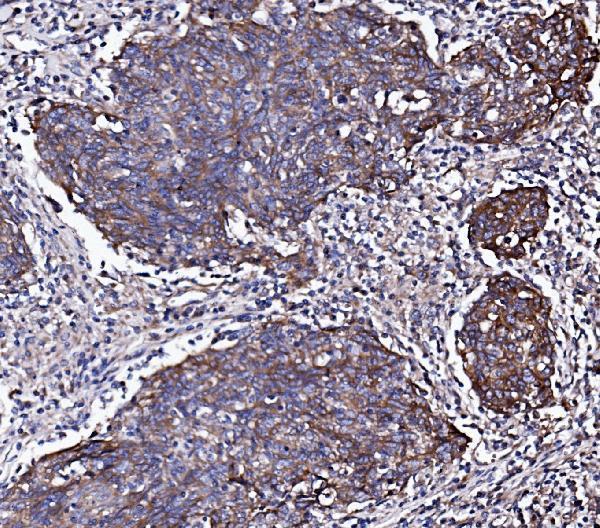
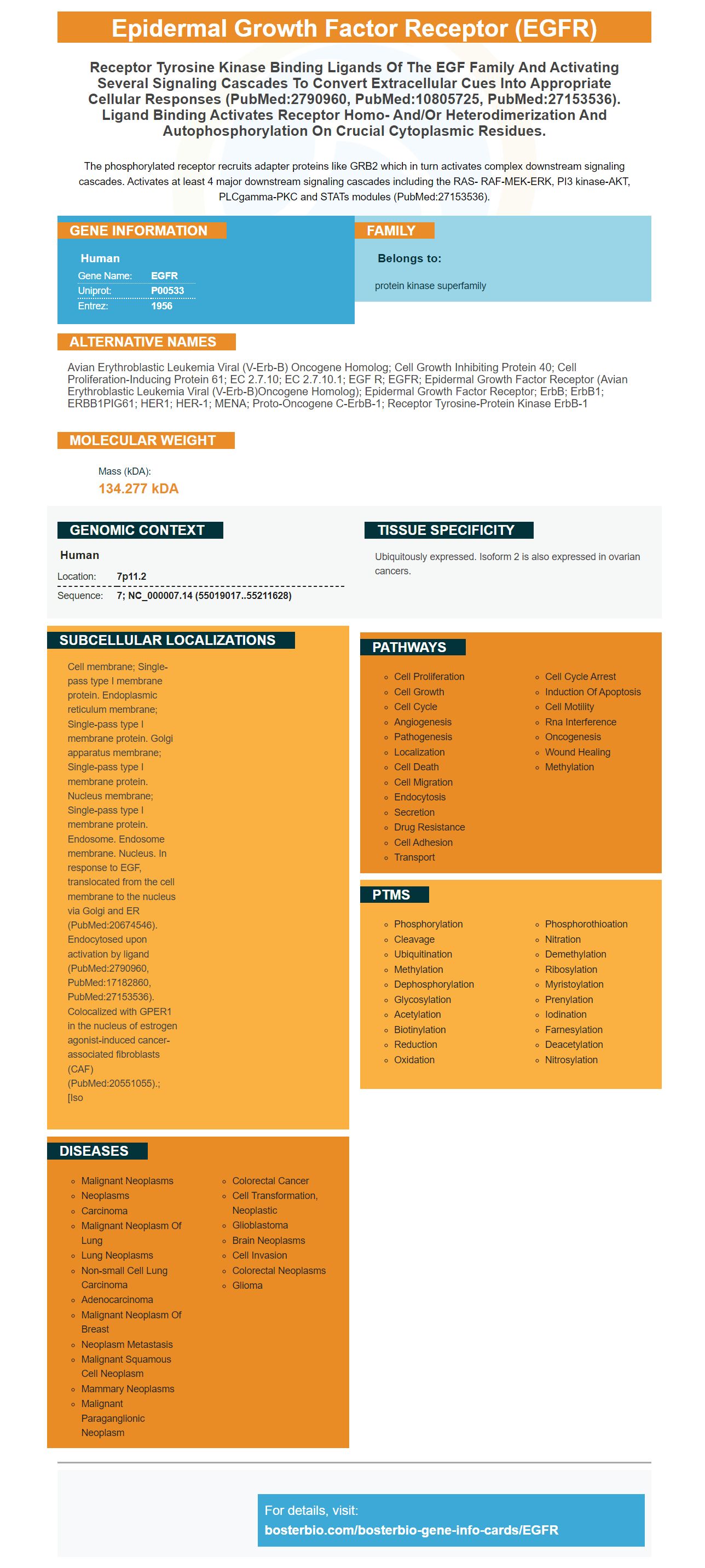
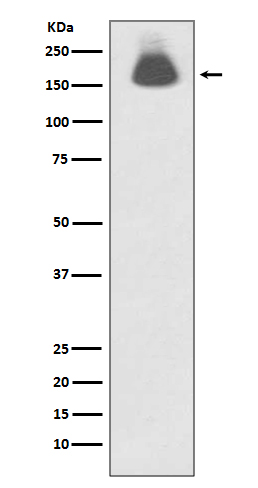
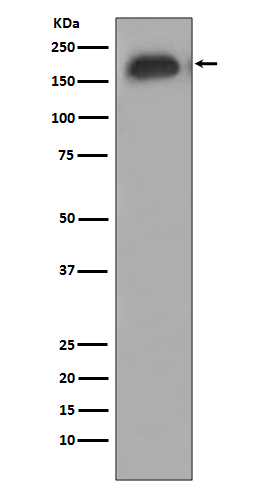
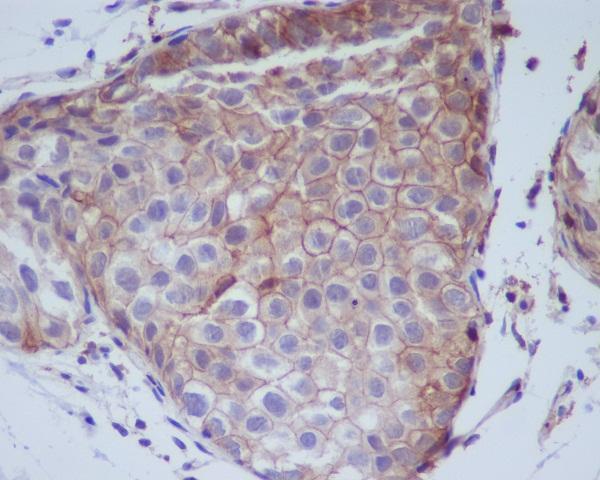
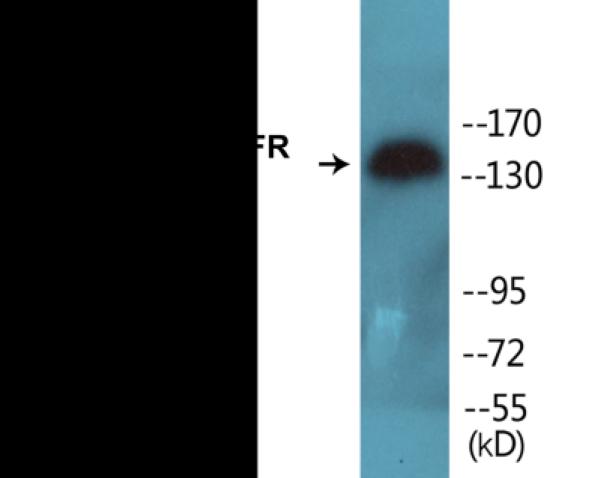
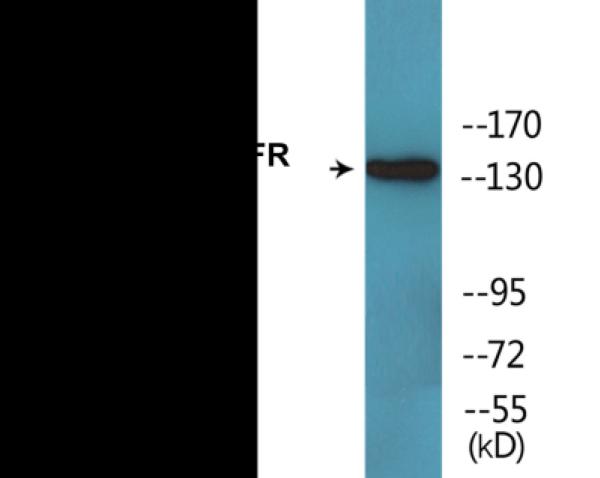
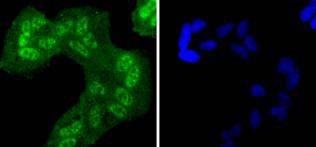
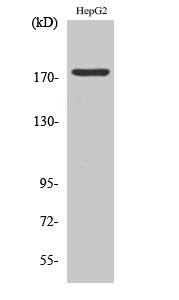
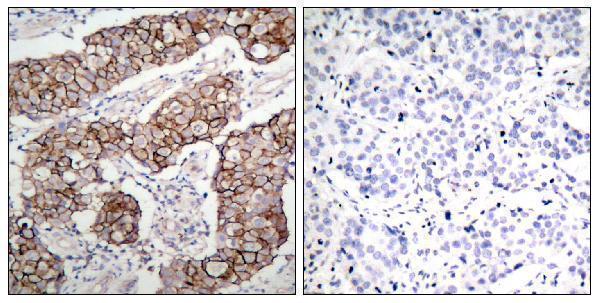
Facts about Epidermal growth factor receptor.

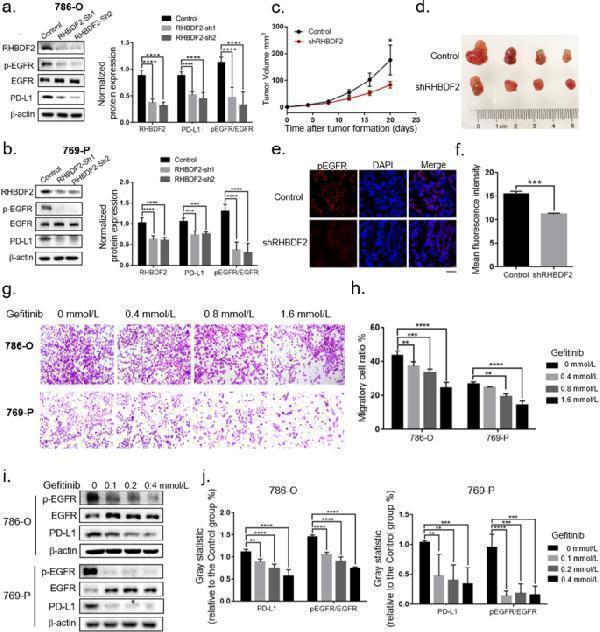
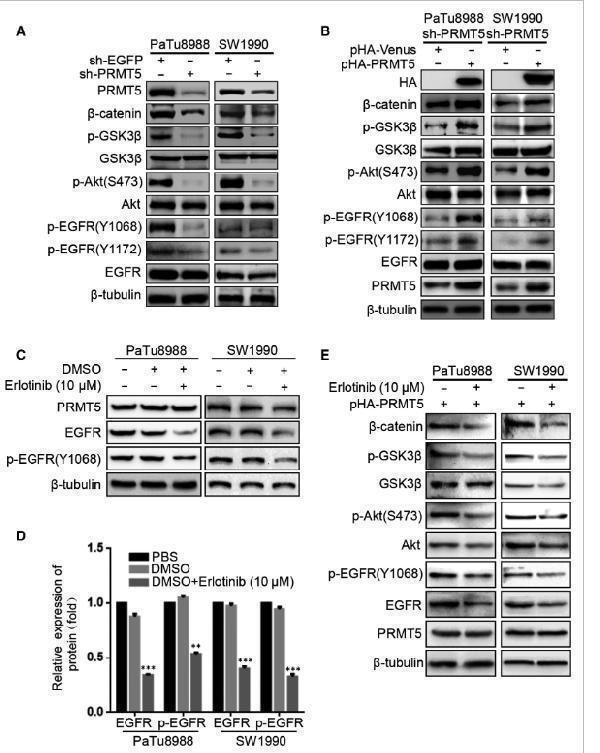
The phosphorylated receptor recruits adapter proteins like GRB2 which in turn activates complex downstream signaling cascades. Activates at least 4 major downstream signaling cascades including the RAS- RAF-MEK-ERK, PI3 kinase-AKT, PLCgamma-PKC and STATs modules (PubMed:27153536).
| Human | |
|---|---|
| Gene Name: | EGFR |
| Uniprot: | P00533 |
| Entrez: | 1956 |

| Belongs to: |
|---|
| protein kinase superfamily |

avian erythroblastic leukemia viral (v-erb-b) oncogene homolog; cell growth inhibiting protein 40; cell proliferation-inducing protein 61; EC 2.7.10; EC 2.7.10.1; EGF R; EGFR; epidermal growth factor receptor (avian erythroblastic leukemia viral (v-erb-b)oncogene homolog); epidermal growth factor receptor; ErbB; ErbB1; ERBB1PIG61; HER1; HER-1; mENA; Proto-oncogene c-ErbB-1; Receptor tyrosine-protein kinase erbB-1
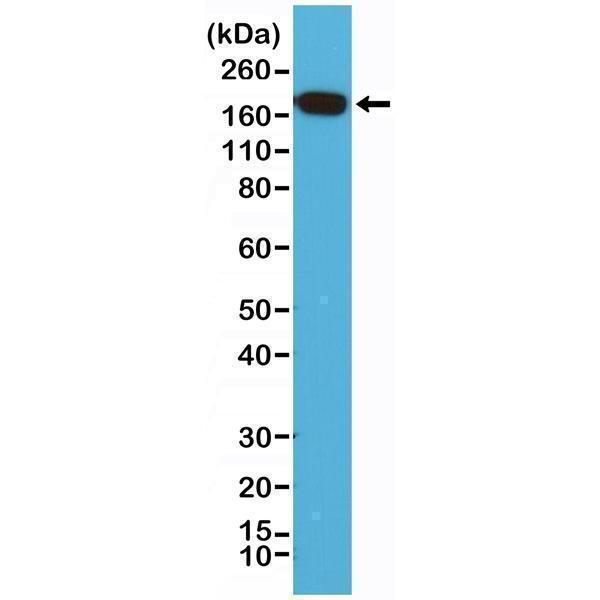
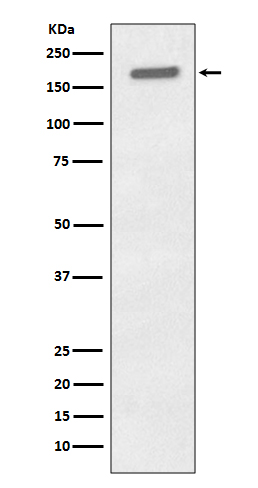
Mass (kDA):
134.277 kDA

| Human | |
|---|---|
| Location: | 7p11.2 |
| Sequence: | 7; NC_000007.14 (55019017..55211628) |
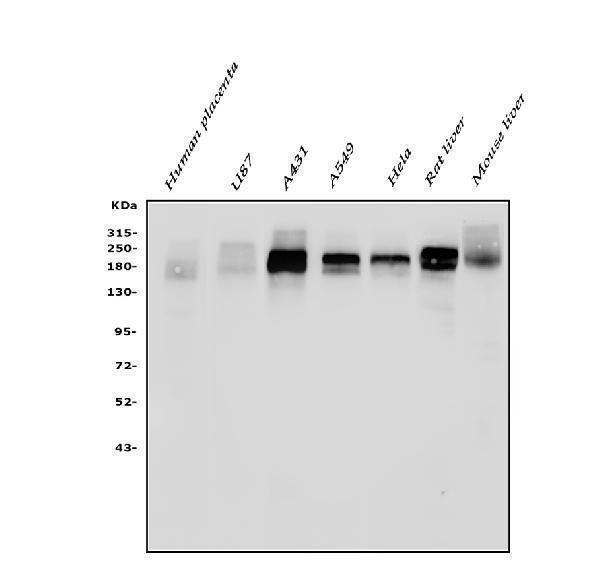
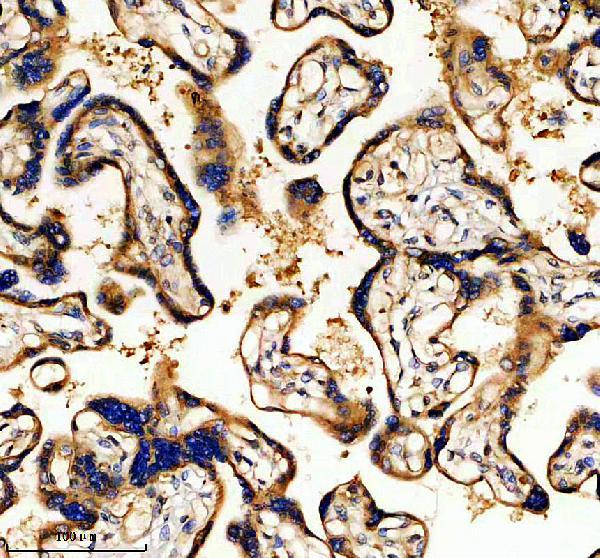
Ubiquitously expressed. Isoform 2 is also expressed in ovarian cancers.
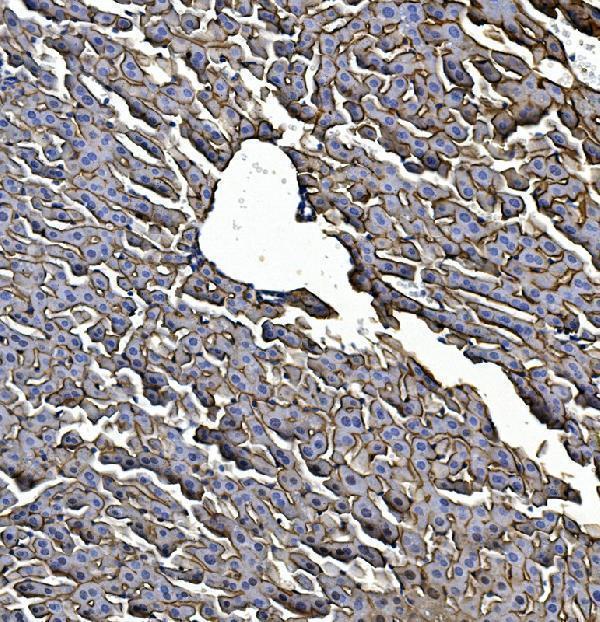
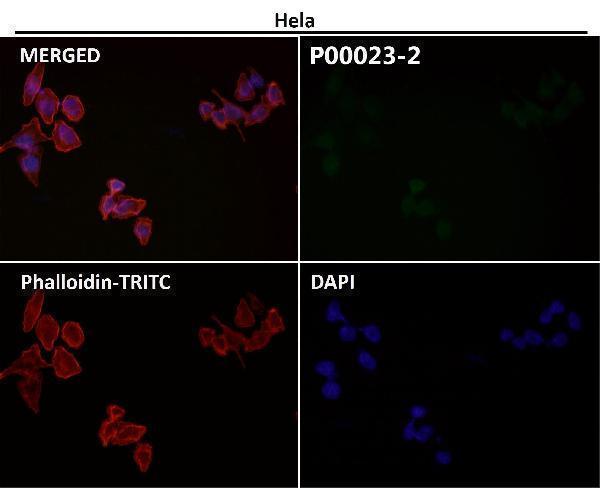
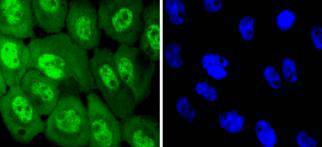
Cell membrane; Single-pass type I membrane protein. Endoplasmic reticulum membrane; Single-pass type I membrane protein. Golgi apparatus membrane; Single-pass type I membrane protein. Nucleus membrane; Single-pass type I membrane protein. Endosome. Endosome membrane. Nucleus. In response to EGF, translocated from the cell membrane to the nucleus via Golgi and ER (PubMed:20674546). Endocytosed upon activation by ligand (PubMed:2790960, PubMed:17182860, PubMed:27153536). Colocalized with GPER1 in the nucleus of estrogen agonist-induced cancer-associated fibroblasts (CAF) (PubMed:20551055).; [Iso



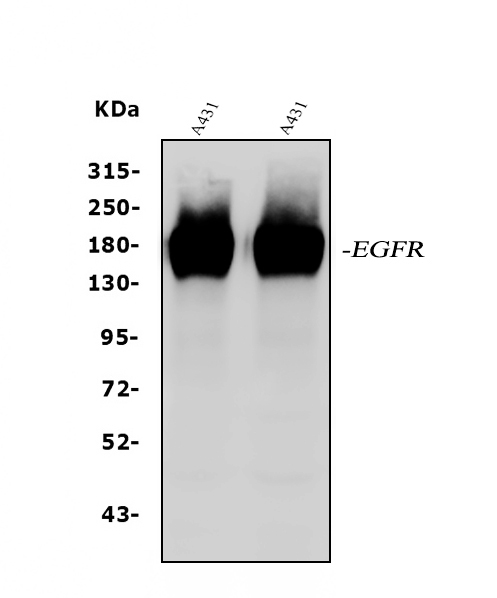
PMID: 6328312 by Ullrich A., et al. Human epidermal growth factor receptor cDNA sequence and aberrant expression of the amplified gene in A431 epidermoid carcinoma cells.
PMID: 7654368 by Ilekis J.V., et al. Possible role of variant RNA transcripts in the regulation of epidermal growth factor receptor expression in human placenta.
*Showing only the more recent 20. More publications can be found for each product on its corresponding product page