This website uses cookies to ensure you get the best experience on our website.
- Table of Contents

A comprehensive resource on using the P53 gene as a biomarker for early cancer diagnosis, reproductive cancer treatment, and CLIA-certified clinical validation.
4 Citations 4 Q&As
3 Citations 9 Q&As

30 Citations 4 Q&As
55 Citations 6 Q&As
1 Citations 4 Q&As
24 Citations 16 Q&As




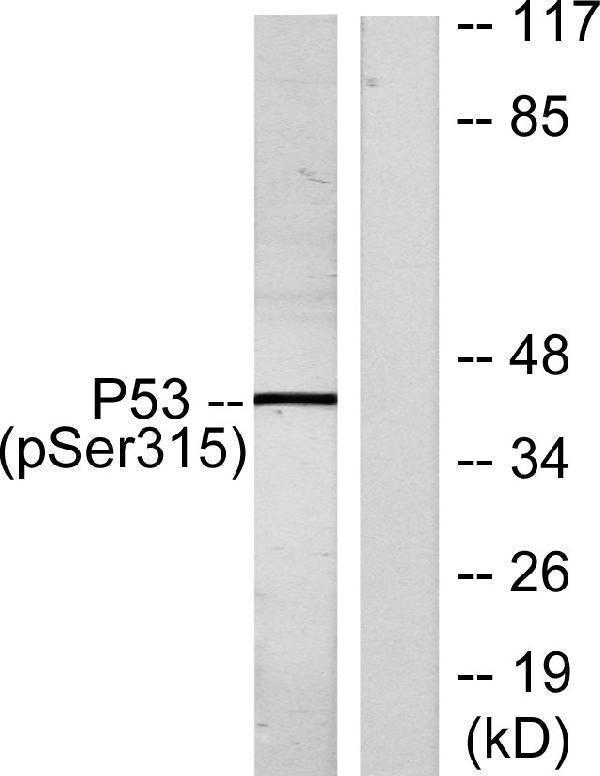
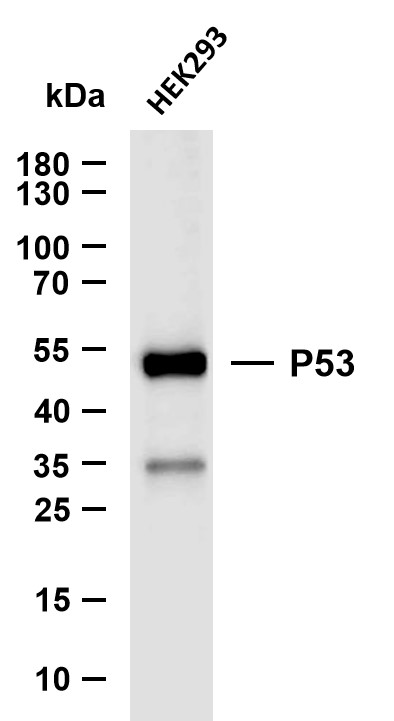
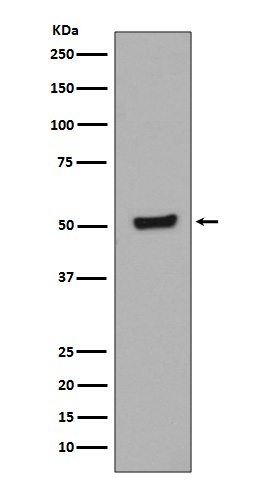
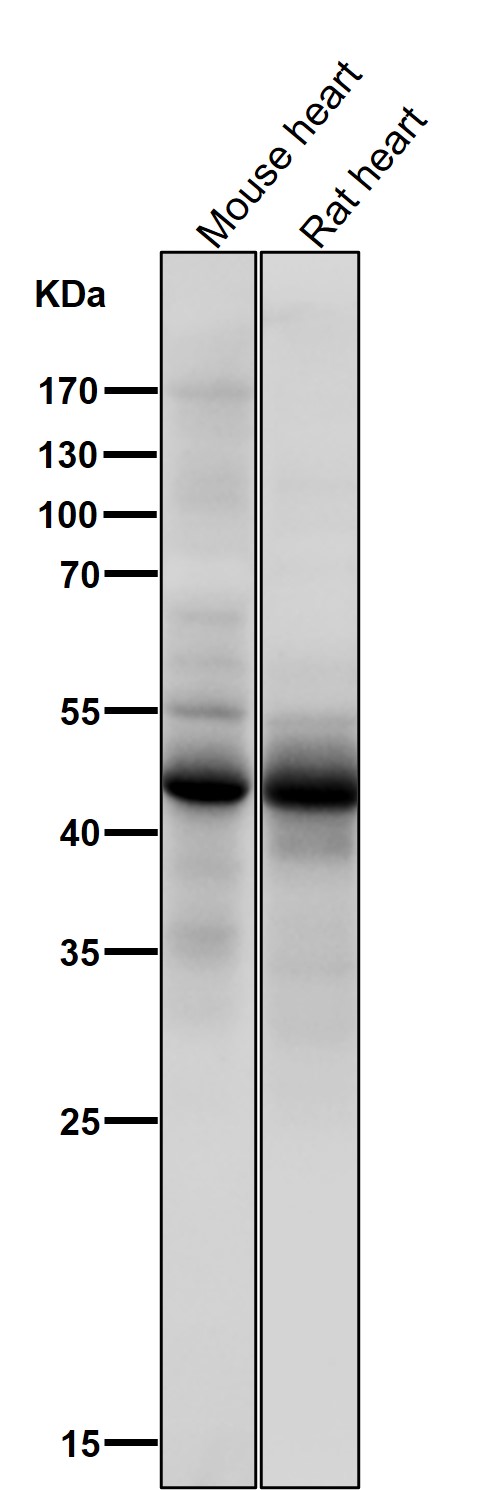
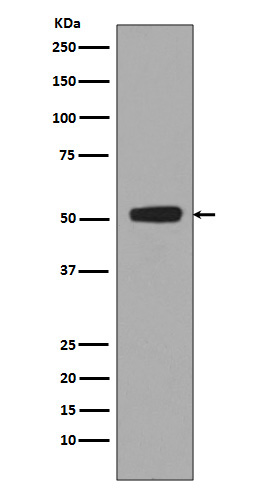
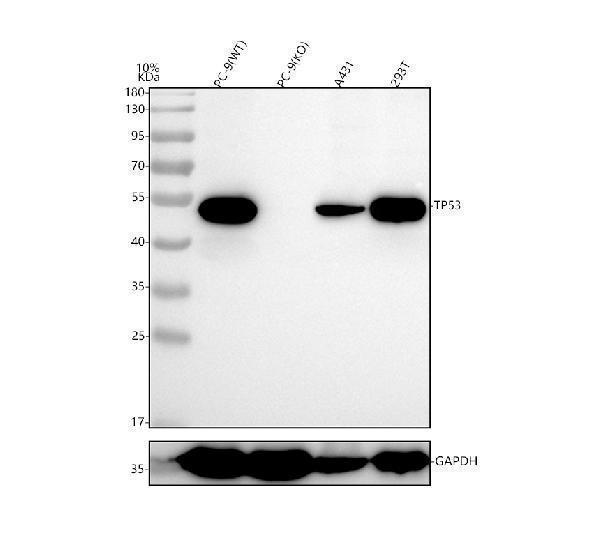
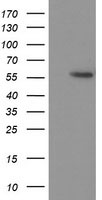
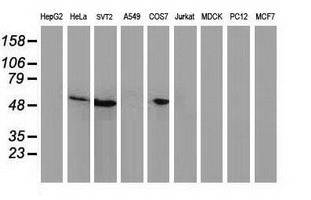
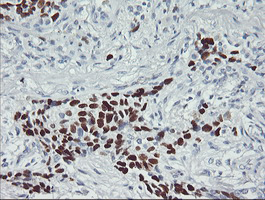
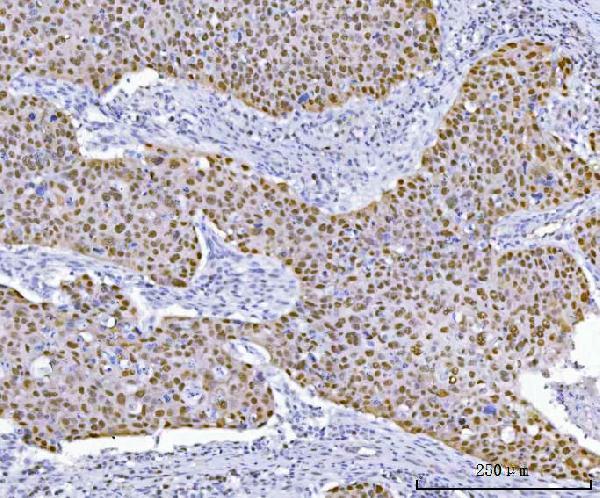
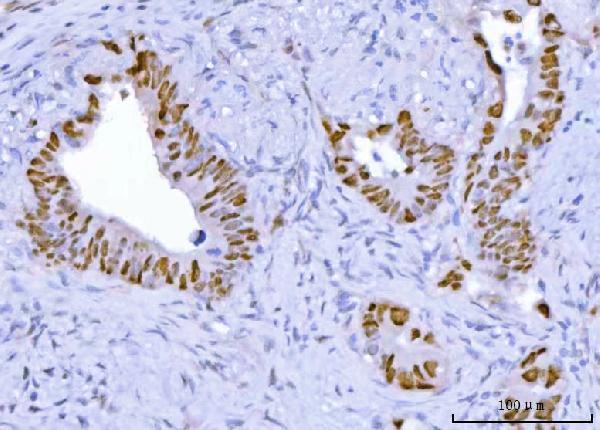
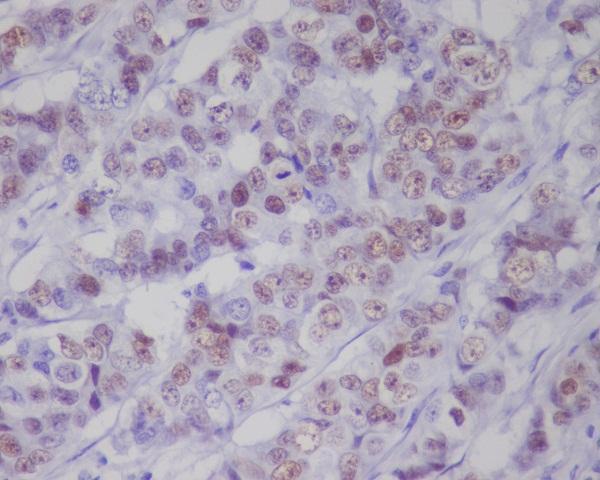
Facts about Cellular tumor antigen p53.

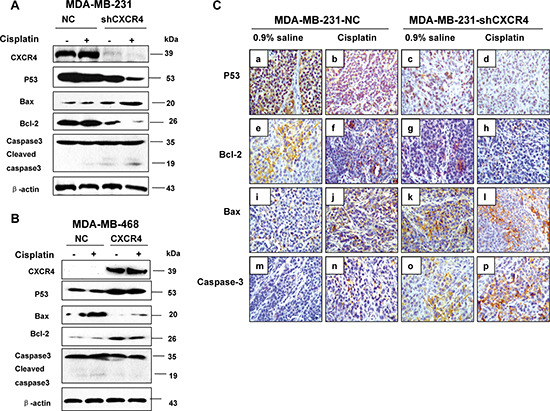
One of the activated genes is an inhibitor of cyclin-dependent kinases. Apoptosis induction seems to be mediated either by stimulation of BAX and FAS antigen expression, or by repression of Bcl-2 expression.
| Human | |
|---|---|
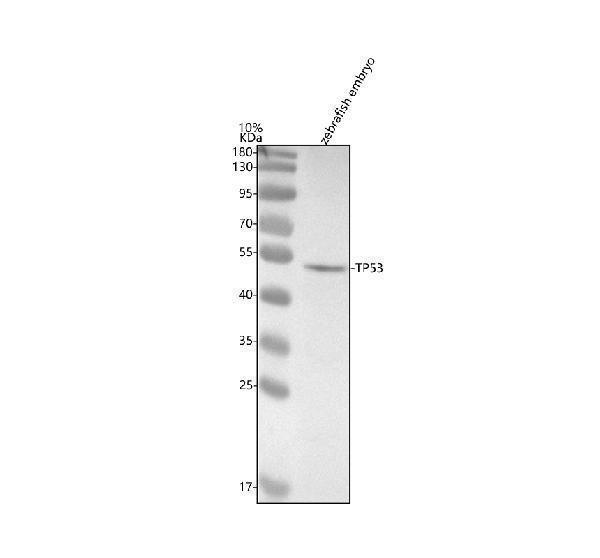
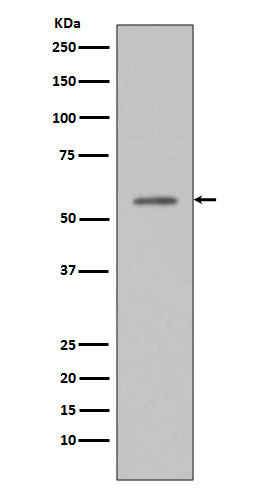
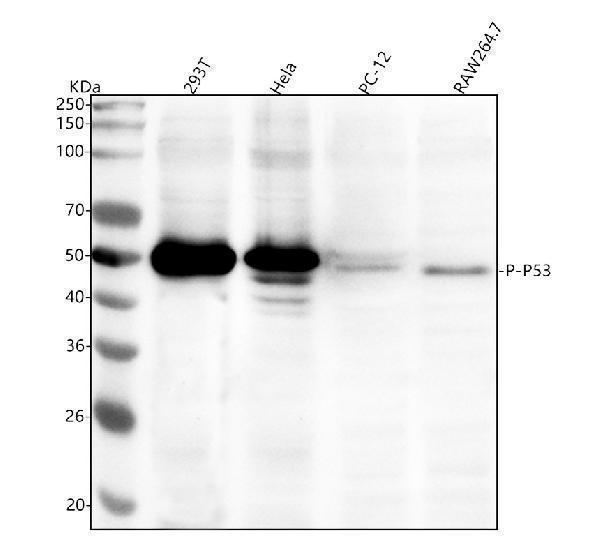
| Gene Name: | TP53 |
| Uniprot: | P04637 |
| Entrez: | 7157 |

| Belongs to: |
|---|
| p53 family |

Antigen NY-CO-13; BCC7; FLJ92943; LFS1; LFS1TRP53; p53 tumor suppressor; p53; P53cellular tumor antigen p53; Phosphoprotein p53; TP53; transformation-related protein 53; TRP53; tumor protein p53; Tumor suppressor p53
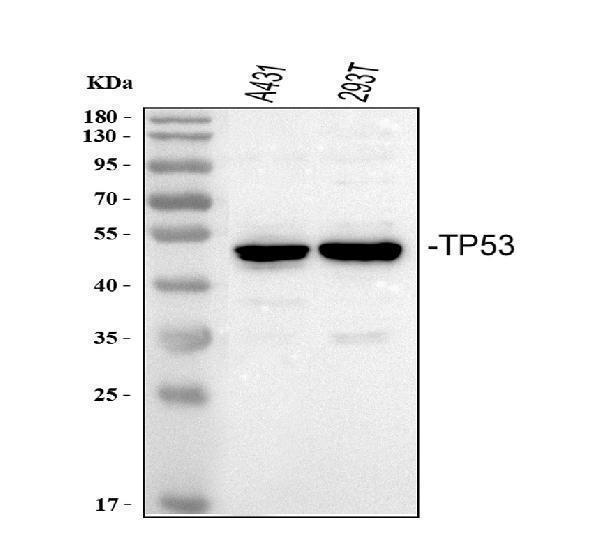
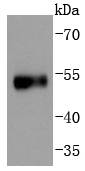
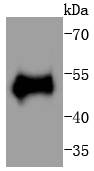
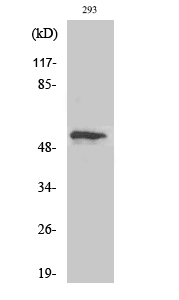
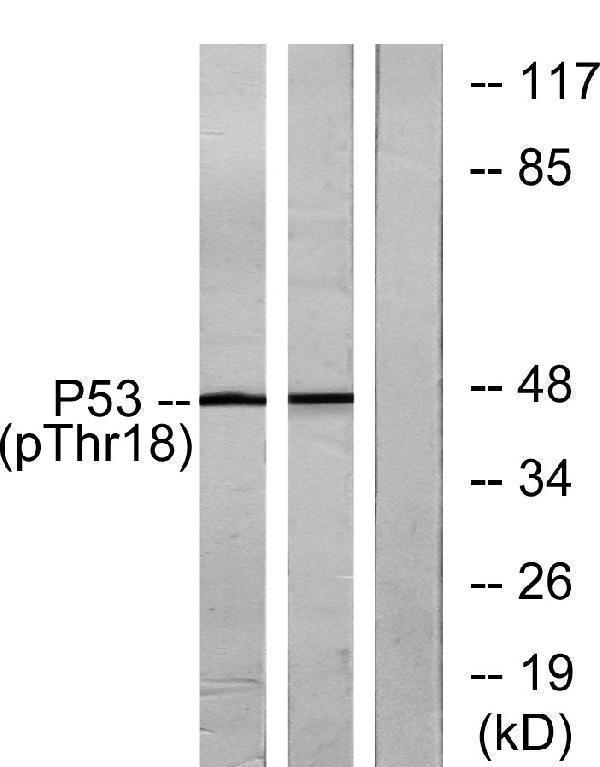
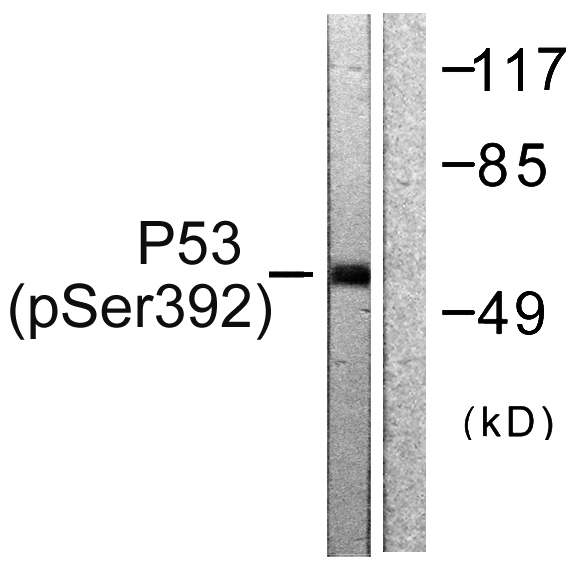
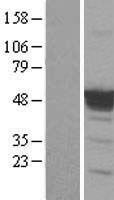
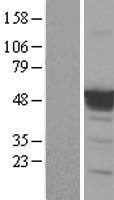
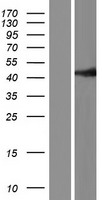
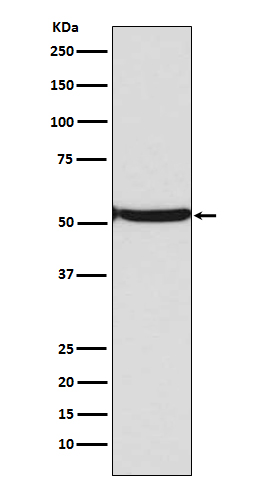
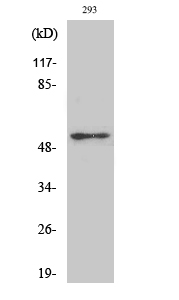
Mass (kDA):
43.653 kDA

| Human | |
|---|---|
| Location: | 17p13.1 |
| Sequence: | 17; NC_000017.11 (7668402..7687550, complement) |
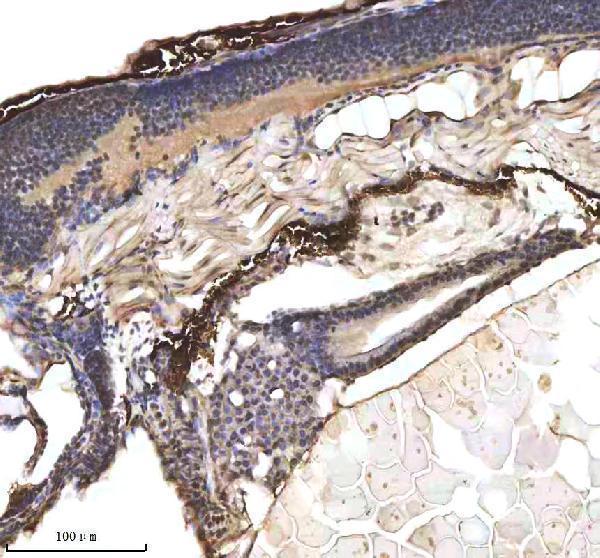
Ubiquitous. Isoforms are expressed in a wide range of normal tissues but in a tissue-dependent manner. Isoform 2 is expressed in most normal tissues but is not detected in brain, lung, prostate, muscle, fetal brain, spinal cord and fetal liver. Isoform 3 is expressed in most normal tissues but is not detected in lung, spleen, testis, fetal brain, spinal cord and fetal liver. Isoform 7 is expressed in most normal tissues but is not detected in prostate, uterus, skeletal muscle and breast. Isoform 8 is detected only in colon, bone marrow, testis, fetal brain and intestine. Isoform 9 is expressed in most normal tissues but is not detected in brain, heart, lung, fetal liver, salivary gland, breast or intestine.
Cytoplasm. Nucleus. Nucleus, PML body. Endoplasmic reticulum. Mitochondrion matrix. Cytoplasm, cytoskeleton, microtubule organizing center, centrosome. Interaction with BANP promotes nuclear localization (PubMed:15701641). Recruited into PML bodies together with CHEK2 (PubMed:12810724). Translocates to mitochondria upon oxidative stress (PubMed:22726440). Translocates to mitochondria in response to mitomycin C treatment (PubMed:27323408).; [Isoform 1]: Nucleus. Cytoplasm. Predominantly nuclear but localizes to the cytoplasm when expressed with isoform 4.; [Isoform 2]: Nucleus. Cytoplasm. Local



PMID: 4006916 by Zakut-Houri R., et al. Human p53 cellular tumor antigen: cDNA sequence and expression in COS cells.
PMID: 2946935 by Lamb P., et al. Characterization of the human p53 gene.
*Showing only the more recent 20. More publications can be found for each product on its corresponding product page