This website uses cookies to ensure you get the best experience on our website.
- Table of Contents

1 Citations
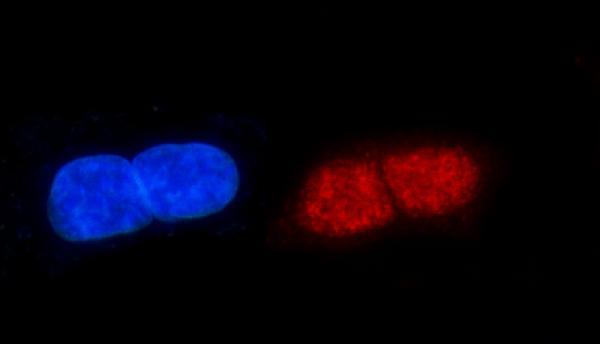
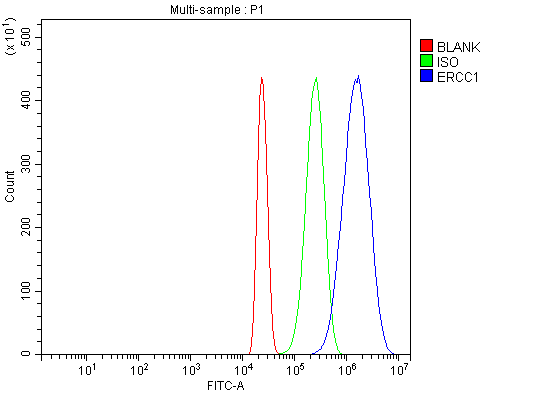
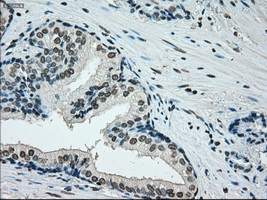
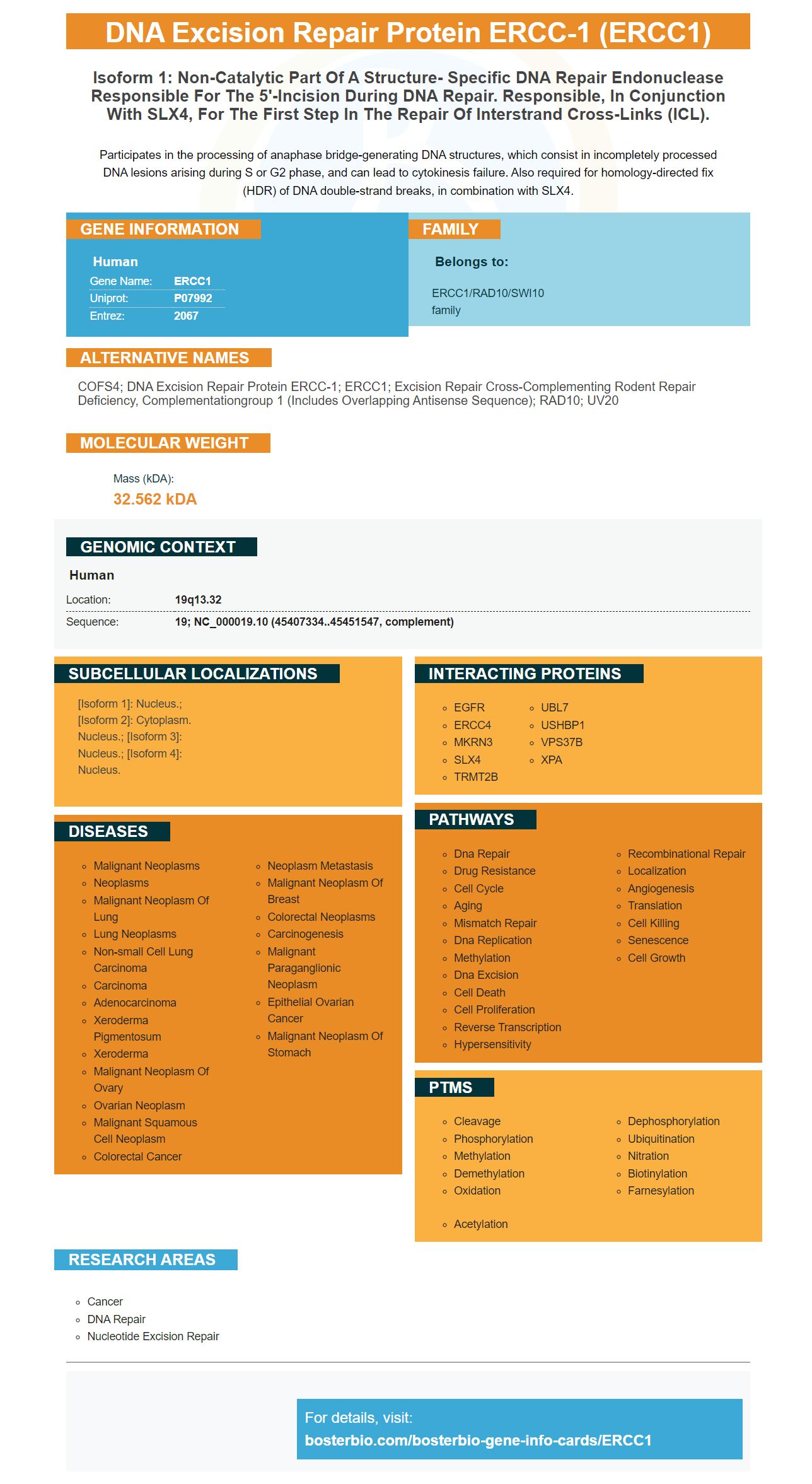
Facts about DNA excision repair protein ERCC-1.

Participates in the processing of anaphase bridge-generating DNA structures, which consist in incompletely processed DNA lesions arising during S or G2 phase, and can lead to cytokinesis failure. Also required for homology-directed fix (HDR) of DNA double-strand breaks, in combination with SLX4.
| Human | |
|---|---|
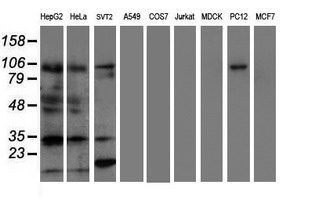
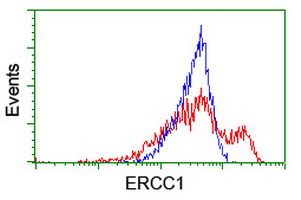
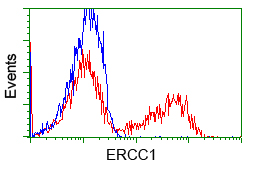
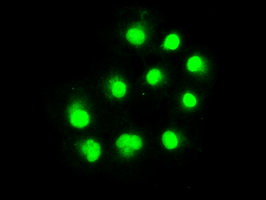
| Gene Name: | ERCC1 |
| Uniprot: | P07992 |
| Entrez: | 2067 |

| Belongs to: |
|---|
| ERCC1/RAD10/SWI10 family |

COFS4; DNA excision repair protein ERCC-1; ERCC1; excision repair cross-complementing rodent repair deficiency, complementationgroup 1 (includes overlapping antisense sequence); RAD10; UV20
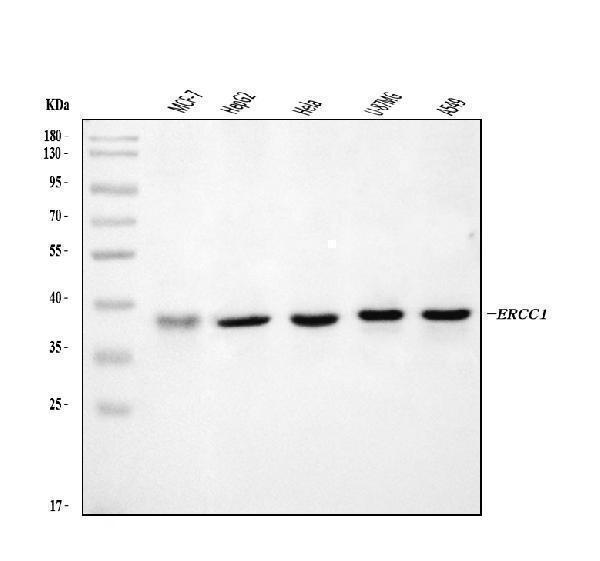
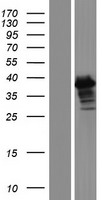
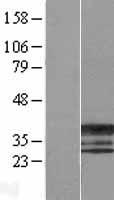
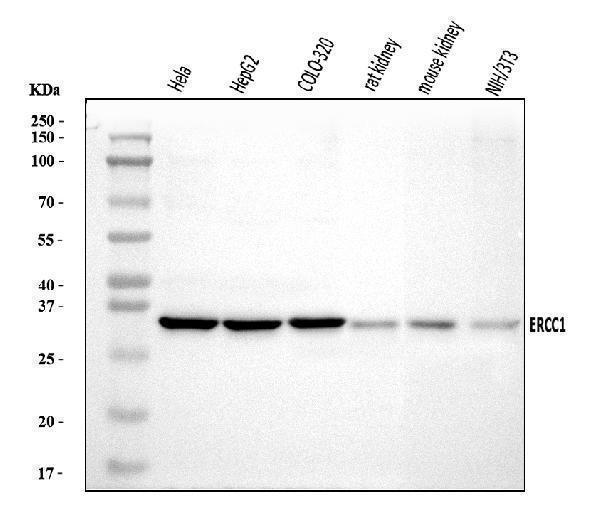
Mass (kDA):
32.562 kDA

| Human | |
|---|---|
| Location: | 19q13.32 |
| Sequence: | 19; NC_000019.10 (45407334..45451547, complement) |
[Isoform 1]: Nucleus.; [Isoform 2]: Cytoplasm. Nucleus.; [Isoform 3]: Nucleus.; [Isoform 4]: Nucleus.




PMID: 2420469 by van Duin M., et al. Molecular characterization of the human excision repair gene ERCC-1: cDNA cloning and amino acid homology with the yeast DNA repair gene RAD10.
PMID: 3034490 by Hoeijmakers J.H.J., et al. Identification of DNA repair genes in the human genome.