This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
Choosing between a monoclonal and a polyclonal primary antibody for IHC is less about picking the “better” antibody type and more about deciding which mistake you can least afford.
A useful first question is: are you more worried about missing a real target, or mistaking background for true staining?
If the risk is missing a difficult or poorly exposed target, a polyclonal antibody may be a useful starting point. If the risk is wrong localization, background, or inconsistent staining, a monoclonal antibody is usually easier to interpret. This article focuses on primary antibody selection for standard IHC using FFPE or frozen tissue sections.
In most workflows, the primary antibody is paired with a secondary antibody that enables signal amplification and visualization. Although this article focuses on choosing the primary reagent, both components influence final staining quality, antigen detection, and overall assay performance.
For broader workflow context, see IHC protocol and IHC technical resource center.
IHC keeps the target inside a tissue section after fixation, embedding, sectioning, and antigen retrieval. That tissue context changes how antibodies behave.
Changes introduced during tissue fixation and processing can alter epitope accessibility, particularly in formalin-fixed sections. As a result, successful staining depends not only on antibody selection but also on preservation of the underlying antigen-antibody interaction required for reliable epitope detection.
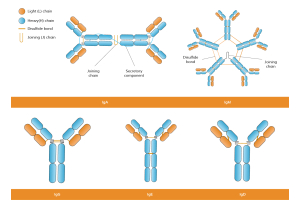
A monoclonal antibody recognizes one epitope. That can be an advantage when the epitope is accessible and the expected pattern is specific. But it also means the antibody depends on that one epitope surviving tissue processing.
A polyclonal antibody recognizes multiple epitopes. That can help when epitope exposure is uneven, the target is low-abundance, or the sample is difficult. But broader recognition can also make background or cross-reactivity harder to separate from true signal.
The practical difference is simple: monoclonal antibodies reduce ambiguity when the epitope is accessible; polyclonal antibodies reduce false-negative risk when epitope exposure is uncertain. If fixation or retrieval is the suspected issue, review antigen retrieval conditions and fixation effects before assuming the antibody format is the only problem.
Choose a monoclonal antibody when the result must be clean, localized, and reproducible.
This is especially important for targets with a defined cellular pattern: nuclear markers should stain nuclei, membrane proteins should show a membrane pattern, and cell-type markers should highlight the expected population.
Many monoclonal antibodies used in research and clinical studies are selected through advanced screening strategies involving antibody libraries, in-vitro display, SPR binning, and characterization of binding behavior. These approaches help identify candidates with strong specificity and appropriate binding specificity and staining performance.
Monoclonal antibodies are also preferable when:
In addition to IHC, antibodies chosen for multiplex panels are often validated using complementary methods such as flow cytometry and western blots to confirm target recognition across different experimental platforms.
For more complex panel design, Boster’s multiplex IHC service page can be a useful next step.
The main caution is that a monoclonal negative is not always a true negative. If the clone’s epitope is masked by fixation or not exposed by the retrieval condition, the target may be present but invisible to that antibody.
This consideration becomes particularly important when evaluating proteins that exist in multiple forms, exhibit an altered antigenic phenotype, or contain an antigenic variant that affects antibody binding.
Start with a polyclonal antibody when detectability is the biggest concern.
This often applies to low-abundance targets, difficult FFPE samples, poorly characterized proteins, or non-model species. Because polyclonal antibodies recognize multiple epitopes, they may still bind when some regions are masked or altered.
Broader recognition can also be advantageous when studying targets associated with a changing immune response or proteins that display heterogeneous structural features.
Polyclonal antibodies can also be useful when validated monoclonal options are limited. Examples include emerging biomarkers, poorly characterized proteins, or certain virus protein targets for which limited validation data are available. For rare species or novel targets, a broader antigen region may improve the chance of recognizing conserved sequences. When no suitable antibody exists, a custom polyclonal antibody development workflow may be more practical than forcing an antibody that was never validated for the sample context.
The trade-off is clear: a stronger stain is not automatically a better stain. Review polyclonal results carefully when the signal is diffuse, appears in unexpected regions, or does not match known biology.
Unexpected staining patterns should always be interpreted alongside available biological evidence, known protein localization, and the expected immune response associated with the target.
A common mistake is to trust the slide that looks strongest. Strong staining alone does not confirm accurate antigen detection. Excessive signal can sometimes reflect off-target binding, especially when localization is inconsistent with established biology. A polyclonal antibody may give intense staining because it binds multiple epitopes, but if the signal appears at tissue edges, in necrotic areas, or in the wrong compartment, the result is unreliable.
A monoclonal antibody may give a weaker but cleaner pattern. For localization studies, that is often more valuable than a strong but messy stain.
For many applications, confidence in localization is more valuable than maximizing signal intensity because it improves interpretation of the underlying antigen-antibody interaction.
Be cautious with broad cytoplasmic haze for membrane targets, cytoplasmic staining for nuclear markers, signal restricted to necrotic or edge regions, staining in known negative tissue, or signal that improves only when background also rises.
If the main problem is weak signal, it may be worth checking Boster’s guide to weak or no staining in IHC. If the problem is background or unexpected staining, review non-specific staining in IHC before switching antibody type.
| IHC Situation | Better Starting Point | Why |
|---|---|---|
| First-pass detection of a difficult target | Polyclonal or multiple clones | Reduces false-negative risk when epitope exposure is uncertain |
| Clear nuclear, membrane, or cell-type localization is needed | Monoclonal | Cleaner pattern is easier to interpret |
| Comparing staining across many samples | Monoclonal | More consistent staining behavior supports comparison across samples |
| Low-abundance target in FFPE tissue | Polyclonal or optimized monoclonal | Detection may depend on epitope recovery |
| Target has close homologs or isoforms | Monoclonal | Defined epitope helps reduce cross-reactivity risk |
| Phospho- or cleavage-specific target | Validated monoclonal often preferred | Must distinguish modified or cleaved form from total protein |
| Rare species or non-model organism | Polyclonal may help | Broader recognition may detect conserved regions |
| Multiplex or multi-marker IHC | Monoclonal often preferred | Reduces ambiguity between markers |
Many principles used in antibody selection for IHC also appear in therapeutic antibody discovery. During antibody development, researchers may use next-generation sequencing, Sanger sequencing, and computational approaches including machine learning to evaluate candidate antibodies and characterize binding properties across large datasets.
These methods can help identify sequence features associated with specificity, stability, and performance. Metrics such as clone abundance or relative frequency within screening campaigns may guide candidate prioritization before functional testing.
Characterization workflows may also assess the effects of antibody fragmentation, interactions with purification reagents such as Protein G, and differences in binding behavior among antibodies recognizing similar targets.
For difficult targets, benchmark more than one antibody instead of committing to one format.
Compare two monoclonal clones targeting different epitopes, or one monoclonal and one polyclonal antibody. This strategy is especially useful when evaluating proteins with multiple antigenic sites or targets that may exhibit biologically relevant variation. If independent antibodies give the same biologically plausible pattern, confidence increases. If they disagree, investigate epitope masking, clone specificity, retrieval conditions, or background.
Never treat a single negative IHC result as proof that the target is absent.
Validation is ultimately an evidence-based process. Data from IHC may be strengthened when supported by orthogonal techniques, molecular analyses, or independent biological observations.
The format helps guide the starting choice, but validation determines whether the staining can be trusted.
Peptide blocking can support specificity but is not absolute proof. Blocking shows the antibody can bind the immunizing peptide—not that the tissue signal comes from the correct endogenous target.
Although IHC is primarily used to evaluate protein expression and localization, antibody performance can be influenced by broader biological factors. Variations in protein structure, post-translational modification, and target abundance may affect recognition by both monoclonal and polyclonal antibodies.
In some research settings, factors such as antibody-mediated immunity, antibody-mediated immune response, antibody-mediated selection, prior immune history, and patterns of antigenic diversification may contribute to differences in target presentation. These concepts are particularly relevant when studying infectious diseases, vaccine responses, or dynamic biological systems.
The prevalence of a target within a study cohort, its effective population size, and assumptions incorporated into a mathematical model may also influence interpretation of validation data and biological significance.
No. Monoclonal antibodies are often better for clean localization, reproducibility, and lower ambiguity, but they can fail if the target epitope is masked during fixation or antigen retrieval.
Not necessarily. A well-validated polyclonal antibody can work well for low-abundance or difficult targets. The concern is that broader recognition can also increase background, so localization and controls matter.
Polyclonal preparations may contain antibodies recognizing different epitopes and isotypes. Depending on the immunization strategy, this can include populations related to IgM antibodies or IgA antibodies, although purified research antibodies are typically optimized for specific applications.
Only after checking the basics. Weak staining can come from fixation, retrieval, antibody dilution, incubation time, detection chemistry, or the wrong positive control. If those are reasonable and epitope exposure is still uncertain, a polyclonal antibody or another clone may help.
Validation matters more. The best antibody is not simply monoclonal or polyclonal. It is the antibody that gives a specific, reproducible, and biologically plausible staining pattern in your tissue and protocol.
Monoclonal antibodies are usually better when you need clean localization, reproducibility, and low interpretation ambiguity. Polyclonal antibodies may help when the target is difficult to detect, epitope exposure is uncertain, or the experiment is exploratory.
In IHC, the right antibody is not the one that gives the strongest signal. It is the one that gives a staining pattern you can interpret and defend.
Whether the antibody originated from screening platforms, advanced antibody libraries, or modern discovery workflows, careful validation remains the most important step in determining suitability for IHC.
For related reagents or project support, explore Boster’s IHC reagents page or the IHC histology services page.