This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
Immunohistochemistry staining delivers spatial context that bulk methods cannot replicate, but every protein detection method carries trade-offs in sensitivity, throughput, and sample compatibility. This review maps out where each approach excels, how to choose the right tool for your study design, and how to avoid the most common method-selection errors in cancer research and longitudinal biomarker studies, particularly in the context of protein quantification methods and protein assay techniques.
Choose immunohistochemistry (IHC) when you need to localize a protein within intact tissue, score expression at the single-cell or compartment level, or work with archival FFPE samples. Use ELISA or mass spectrometry when you need precise absolute quantification from cell lysates or serum. Use immunofluorescence (IF) when multiplexing four or more markers on the same section. The right choice depends on three variables: your sample type, whether spatial context is scientifically necessary, and how your data will drive downstream decisions such as treatment selection or biomarker validation.
Figure 1. Schematic overview of the standard immunohistochemistry procedure on FFPE tissue, illustrating antigen-antibody binding and enzyme-mediated chromogenic detection. Spatial localization of signal within cellular compartments is preserved throughout.
Choosing between immunohistochemistry and alternative protein detection methods is rarely a simple binary decision. Each approach interrogates protein biology from a different vantage point, including protein structure, protein–protein interactions, and broader biological processes such as cell signaling and enzymatic catalysis.
While IHC provides spatial localization, bulk techniques such as enzyme-linked immunosorbent assay and mass spectrometry focus on protein quantification and protein quantitation. These methods often rely on protein assays to measure protein concentration in lysates or serum samples.
ELISA, for example, depends on a standard curve generated from known concentrations of the target analyte, enabling accurate protein quantification methods in high-throughput workflows using plate reader systems or microplate readers.
Immunohistochemistry staining is the only widely adopted protein detection method that simultaneously preserves tissue morphology, enables single-cell resolution, and integrates directly with routine pathology workflows. This makes it indispensable for immunohistochemistry cancer diagnosis and biomarker-driven treatment selection.
When researchers ask "why is an IHC test required," the answer usually involves one of three needs: anatomical localization of a protein biomarker, regulatory-pathway histopathological confirmation (e.g., HER2 in breast cancer), or retrospective analysis of archival FFPE tissue unavailable to proteomics workflows.
| Method | Detects | Spatial Info | Quantitation | Sample Type | Throughput | Best For |
|---|---|---|---|---|---|---|
| IHC (chromogenic) | Protein (in situ) | Yes | Semi-quant. | FFPE, Frozen | Moderate | Histopathology, biomarker dx, cancer grading |
| IF / IHC fluorescence | Protein (in situ) | Yes | Semi-quant. | Frozen, cells, FFPE | Moderate | Multiplexing, subcellular co-localization |
| ELISA | Protein (bulk) | No | Quantitative | Serum, CS, lysate | High | Serum biomarker quantification, drug monitoring |
| Western Blot | Protein (bulk) | No | Semi-quant. | Lysate | Low | Antibody validation, PTM detection, molecular weight |
| Mass Spectrometry | Protein (bulk) | Emerging | Highly quant. | Lysate, FFPE digest | Low–Med | Proteome-wide discovery, PTM profiling |
| ISH / RNAscope | mRNA (in situ) | Yes | Semi-quant. | FFPE, Frozen | Low | Gene expression at single-cell resolution |
| Flow Cytometry | Protein (single cells) | No | Quantitative | Single-cell suspension | High | Immune phenotyping, live/dead cell discrimination |
| RT-qPCR | mRNA | No | Quantitative | RNA extract | High | Gene expression quantification, companion diagnostics |
Table 1. Cross-method comparison of IHC methods and alternative protein/gene detection approaches. PTM = post-translational modification; Dx = diagnosis.
Note: ISH/RNAscope and RT-qPCR detect RNA rather than protein, but they are included because they are commonly used alongside IHC to compare protein localization with gene expression patterns.
Sample preparation determines which protein assay techniques are feasible. For bulk assays, protein extraction is required to isolate proteins from cells or tissues, which disrupts spatial context but enables downstream applications such as protein purification and quantitative analysis.
Protein detection methods based on absorbance often rely on UV light to measure peptide bonds, since the peptide bond absorbs strongly at 280 nm due to aromatic amino acids. Colorimetric assays such as those using Coomassie dye (e.g., Bradford assay) are widely used in Protein Assays for rapid estimation of protein concentration.
The immunohistochemistry protocol for frozen sections skips chemical fixation and antigen retrieval, preserving labile epitopes and enzymatic activity. However, morphology suffers, storage is demanding, and pre-surgical planning is required to snap-freeze fresh tissue. For longitudinal disease progression studies where samples were collected over years, FFPE is almost always the only available format.
| Parameter | FFPE Tissue | Frozen Tissue | Cell Culture (ICC) |
|---|---|---|---|
| Morphology preservation | Excellent | Good | Excellent |
| Antigen retrieval needed | Yes (HIER/PIER) | Usually No | Usually No |
| Labile epitope access | Variable | Excellent | Excellent |
| Archival compatibility | Yes (decades) | Limited | Limited |
| RNA co-detection (ISH) | Partial | Yes | Yes |
| Suitable for multiplexed IHC | Yes (most platforms) | Select platforms | IF preferred |
For cell-based applications such as the ICC protocol for cell culture, many researchers opt for immunofluorescence rather than chromogenic IHC. Cultured cells lack the tissue architecture that makes spatial context meaningful in IHC, but fluorescence labeling offers easy multiplexing and subcellular co-localization without requiring sectioning.
Cross-linking fixatives (formaldehyde, glutaraldehyde) and coagulant fixatives (ethanol, methanol, acetone) alter epitope accessibility differently. Antibody clones validated on alcohol-fixed tissue may fail on FFPE without optimization of antigen retrieval conditions (pH, temperature, buffer composition). Always confirm fixation compatibility before implementing a new immunohistochemistry procedure.
Mass spectrometry offers highly sensitive detection and supports drug development workflows by enabling large-scale protein quantification across complex samples. However, it requires prior protein extraction, eliminating spatial information.
In contrast, IHC enables visualization of proteins in situ without disrupting tissue architecture. This makes it indispensable for studying protein–protein interactions within the tumor microenvironment and for validating targets identified during drug development.
Advanced analytical approaches now integrate machine learning to correlate spatial IHC data with proteomic datasets, improving interpretation of complex biological patterns.
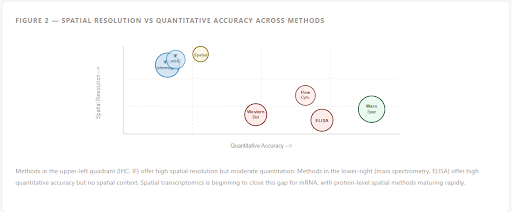
Figure 2 — Spatial Resolution vs Quantitative Accuracy Across Methods
Methods in the upper-left quadrant (IHC, IF) offer high spatial resolution but moderate quantitation. Methods in the lower-right (mass spectrometry, ELISA) offer high quantitative accuracy but no spatial context. Spatial transcriptomics is beginning to close this gap for mRNA, with protein-level spatial methods maturing rapidly.
For longitudinal disease progression studies, IHC is often the method of first resort because it permits retrospective cohort analysis on archival tissue and enables the researcher to correlate morphological changes with protein expression shifts in the same section. Mass spectrometry can complement this by providing absolute abundance data from matched laser-captured microdissected regions, creating a multi-modal dataset that neither technique could produce alone.
IHC remains central in clinical workflows due to its compatibility with antibody-based detection and its ability to assess biomarker localization. In contrast, assays such as ELISA rely on bulk detection using calibrated standard curve models. In research settings, fluorescent labeling techniques using fluorescent proteins such as green fluorescent protein enable visualization of dynamic biological processes, although these are typically applied in live-cell imaging rather than FFPE tissue analysis.
The immunohistochemistry principle applies across a wide range of diagnostic and research contexts. The scenarios below illustrate when the method genuinely outperforms alternatives and when a complementary approach would strengthen your data.
HER2, ER, PR, PD-L1, and ALK are all assessed by immunohistochemical staining in routine oncology. The IHC test provides spatial scoring (H-score, Allred score) that directly informs therapy selection. An IHC test positive result for PD-L1 guides checkpoint inhibitor eligibility; IHC test negative for ER shifts breast cancer treatment toward chemotherapy or targeted agents. Although RNA-based and proteomic assays can provide complementary information, they generally do not replace guideline-established IHC scoring for these routine pathology endpoints.
Retrospective studies tracking tumor microenvironment changes over years of treatment depend on FFPE-compatible assays. IHC enables quantification of immune infiltration (CD8+ T-cells, FOXp3+ Tregs), proliferation index (Ki-67), and apoptosis (cleaved caspase-3) across matched pre- and post-treatment biopsies. This is one of the immunohistochemistry uses that mass spectrometry cannot replicate without extensive sample preparation from archival material.
Understanding spatial relationships between tumor cells, stroma, vasculature, and immune infiltrates requires in situ detection. IHC-based cell density maps and proximity analysis (e.g., distance of CD8+ cells to tumor cells) provide immune contexture data predictive of immunotherapy response. Bulk ELISA or flow cytometry of dissociated tumors loses this spatial structure entirely.
IHC confirms that a target protein is expressed at the intended tissue site before moving to in vivo pharmacological studies. Combined with Western blot to confirm antibody specificity, IHC ensures on-target engagement. The immunohistochemistry procedure can be adapted to xenograft, PDX, and genetically engineered mouse models using species-cross-reactive antibodies.
An IHC test is a method, not a diagnosis. An IHC test for cancer biomarkers (e.g., CK7, CK20, CDX2, TTF-1) helps classify tumor histology and primary site, but the clinical interpretation of a positive or negative result always requires integration with morphology, clinical context, and other investigations. Researchers and clinicians should not conflate the test with the conclusion it supports.
One of the most significant practical advantages of immunofluorescence (IF) over traditional chromogenic IHC is panel multiplexing. By assigning spectrally distinct fluorophores to different antibodies, IF permits simultaneous detection of four to eight protein targets on a single tissue section with full co-localization analysis. This is why the relationship between immunohistochemistry vs immunofluorescence is not simply one of method equivalence: they are complementary tools serving different analytical questions.
Double staining with two chromogens (e.g., DAB producing brown signal and Permanent Red or FastRed producing a red signal) allows concurrent detection of two antigens on a single section. This is sufficient for evaluating phenotypic co-expression (e.g., PD-L1 on tumor cells vs macrophages) or cell-type identification without requiring a fluorescence microscope. The immunohistochemical staining workflow for double staining requires careful sequential antibody application, enzyme inactivation between steps, and chromogen selection optimized for spectral separation under brightfield imaging.
| Strategy | Max Targets / Section | Detection Mode | Equipment Required | FFPE Compatible | Ideal Use |
|---|---|---|---|---|---|
| Single IHC (DAB) | 1 | Brightfield | Standard microscope | Yes | Routine biomarker scoring |
| Double IHC (2 chromogens) | 2 | Brightfield | Standard microscope | Yes | Co-expression, cell typing |
| Multiplex IF (Opal/TSA) | 4–8 | Fluorescence | Multispectral imager | Yes | Immune contexture, TME panels |
| CODEX / PhenoCycler | 40+ | Cyclic IF | Specialized system | Yes | Spatial proteomics, cell atlas |
| Digital Spatial Profiling (DSP) | 40–100 | NanoString / UV | GeoMx system | Yes | Region-of-interest protein/RNA profiling |
| Standard IF (ICC) | 3–5 | Fluorescence | Fluorescence microscope | N/A for ICC | Subcellular co-localization in cultured cells |
Because each TSA round uses a unique fluorophore-conjugated tyramide and antibody stripping occurs between rounds, you can run sequential rounds of primary antibody application on a single FFPE section without spectral bleed-through.
IHC fluorescence (multiplex IF) provides superior multiplexing capacity, quantitative fluorescence intensity per cell, and compatibility with AI-driven image analysis pipelines. Chromogenic IHC retains advantages in archival tissue with high autofluorescence, regulatory familiarity, and the ability to simultaneously review morphology under standard brightfield optics alongside a pathologist without specialist imaging equipment.
Specialized multiplex IHC servicesand panel design support are available for longitudinal biomarker studies. Explore validated panels for tumor microenvironment profiling, immune contexture scoring, and companion diagnostic development.
The immunohistochemistry principle requires that antibody-antigen binding produces a detectable signal. In practice, the signal-generation step and antibody format you choose determine your assay's sensitivity, specificity, and compatibility with multiplexing.
Monoclonal antibodies (mAbs) offer superior specificity and lot-to-lot reproducibility, making them the standard for immunohistochemistry cancer biomarker testing and any study requiring inter-laboratory comparison. Polyclonal antibodies (pAbs) provide higher sensitivity for low-abundance targets but introduce cross-reactivity risks that must be controlled with appropriate blocking steps and negative controls. Recombinant antibodies (rabbit monoclonal, human monoclonal) increasingly replace conventional hybridoma-derived clones in critical applications such as the IHC protocol for carrier-free IgG formats.

Figure 3 — IHC Detection System Architecture
Standard indirect IHC uses a secondary antibody conjugated to HRP or alkaline phosphatase. These enzymes react with chromogenic substrates such as DAB, AEC, or Permanent Red to produce a colored precipitate. Polymer-based detection systems eliminate the avidin-biotin step and reduce endogenous biotin interference common in liver, kidney, and adipose tissue. TSA tyramide amplification provides the highest signal-to-noise and is the foundation of multiplex IF platforms.
For multiplexed IHC using sequential rounds, antibody stripping between rounds (microwave or chemical) must be validated for each primary antibody clone to ensure complete removal without section loss. The immunohistochemistry staining procedure for multiplex panels may require custom antibody conjugation or directly conjugated clones to eliminate secondary antibody cross-reactivity.
Turnaround time and total hands-on effort vary enormously across protein detection methods. For a biomedical researcher planning a longitudinal study, these parameters directly affect study timeline, cost, and the volume of samples that can be processed per batch. The immunohistochemistry protocol steps for a standard FFPE staining run from tissue retrieval to scanned slide in 1–2 working days for an experienced laboratory.
Sectioning and Slide Preparation
Sectioning at 4–5 μm; baking at 60°C. ~2 hours; dewaxing; rehydration.
Antigen Retrieval
HIER (heat-induced, citrate pH 6 or Tris-EDTA pH 9) or PIER (enzymatic). 20–40 min.
Blocking
Endogenous peroxidase quenching; serum or BSA block to reduce non-specific background. 30 min.
Primary Antibody
Incubation at optimized dilution; 1 hour RT or overnight 4°C for low-abundance targets.
Secondary Detection
HRP-conjugated secondary or polymer system; 30–60 min incubation.
Chromogen / Counterstain
DAB application (2–10 min); hematoxylin counterstain; dehydration and coverslipping.
| Method | Hands-On Time | Total Turnaround | Automation Available | Batch Scalability |
|---|---|---|---|---|
| IHC (manual) | 3–5 hrs | 1–2 days | Yes (Leica, Ventana, Dako) | 20–60 slides/run |
| IHC (automated) | 1–2 hrs | Same day | Yes | 60–200+ slides/run |
| Multiplex IF (Opal) | 6–12 hrs | 2–4 days | Partial | 4–24 slides/run |
| ELISA | 2–4 hrs | 1 day | Yes | 96–384 wells/plate |
| Western Blot | 6–10 hrs | 1–2 days | Semi (electrophoresis) | 10–20 samples/gel |
| Mass Spectrometry | 8–24 hrs (prep) | 3–7 days | Partial | Low–moderate |
| Flow Cytometry | 3–5 hrs | Same day | Semi | Moderate (requires live cells or rapid processing) |
For high-throughput biomarker validation studies, automated IHC platforms offer the best balance of throughput, standardization, and regulatory traceability. Protocols developed on these systems can be more readily transferred to clinical diagnostic labs, making automated IHC the preferred route for companion diagnostic development and biomarker validation programs.
Sensitivity (ability to detect true positives) and specificity (ability to avoid false positives) are not fixed properties of IHC—they are outcomes of your reagent choices, protocol optimization, tissue preparation, and interpretation strategy. The same target protein can show dramatically different staining patterns depending on antibody clone, antigen retrieval condition, and detection amplification system used in your immunohistochemistry procedure.
Antigen retrieval stringency: Insufficient retrieval is the leading cause of false-negative IHC. The optimal buffer pH (citrate pH 6.0 vs. Tris-EDTA pH 9.0) is epitope-dependent and must be empirically determined.
Antibody dilution: Underdiluted antibodies cause high background; overdiluted antibodies cause weak or absent signal. Titration across a 4–5-point dilution range is mandatory for new antibody-tissue combinations.
Detection amplification: Tyramide signal amplification increases detection sensitivity by 100–1000x compared to standard indirect IHC, enabling detection of very low-abundance proteins such as nuclear transcription factors.
Controls: A validated IHC protocol includes positive tissue control (known-positive tissue), negative reagent control (omit primary antibody), and isotype control to distinguish specific from non-specific staining.
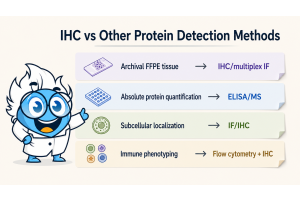
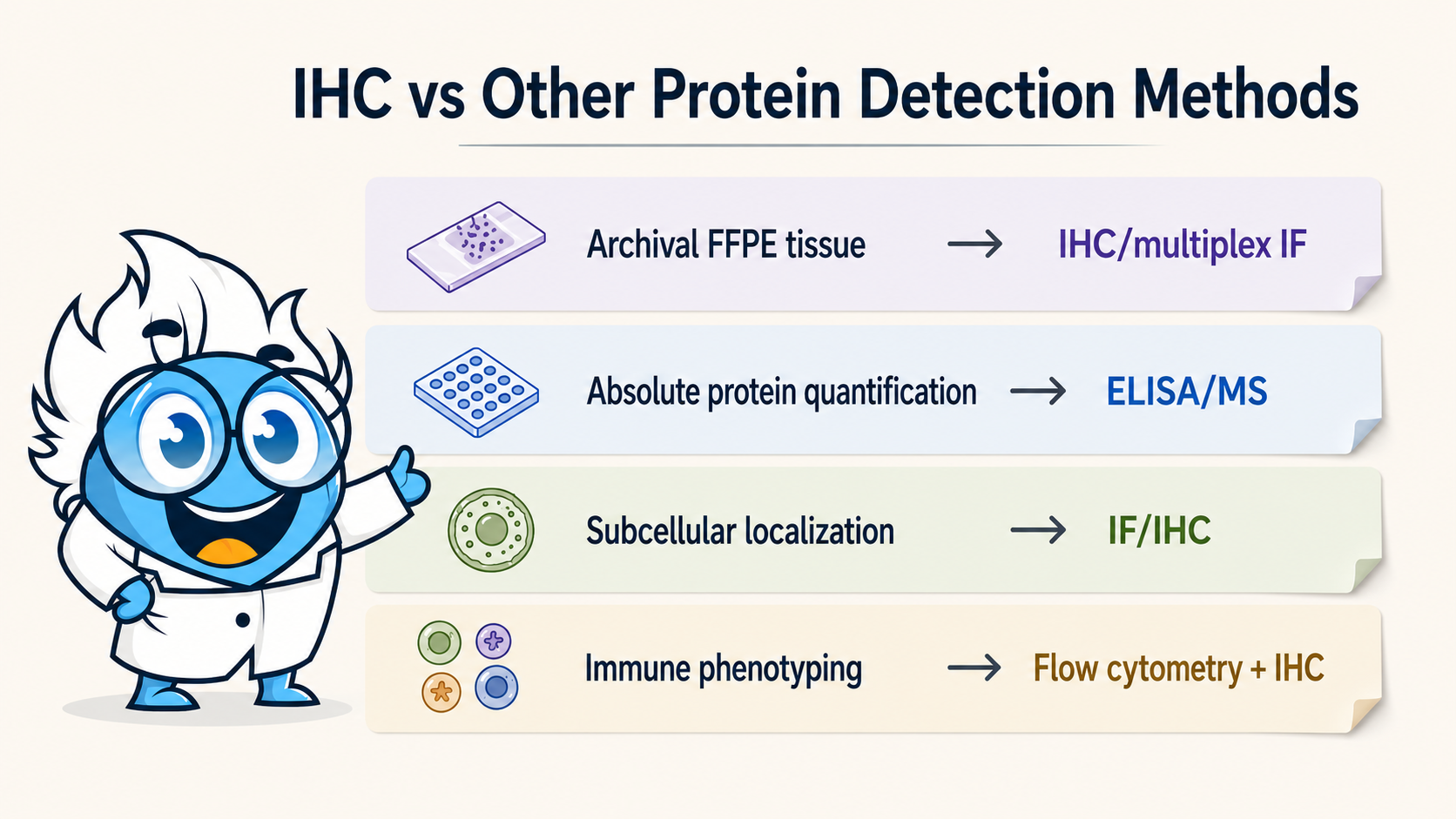
Method selection should work backward from the decision or output your data needs to support. A biomarker that will ultimately inform treatment selection must meet a different evidence bar than a discovery-phase protein expression survey. The following decision framework helps researchers match assay choice to downstream application.
Need archival FFPE tissue?
IHC or multiplex IF
Need absolute protein quantification?
ELISA or mass spectrometry
Need subcellular localization?
IHC or IF (fluorescence)
Regulatory / companion diagnostic?
Validated IHC (CLIA/CE-IVD)
Proteome-wide discovery?
Mass spectrometry
Immune cell phenotyping?
Flow cytometry + IHC for spatial validation
Single-cell spatial proteomics?
CODEX / PhenoCycler / DSP
For biomarker validation pipelines, the standard approach is a staged workflow: initial discovery via mass spectrometry or transcriptomics identifies candidate proteins; ELISA confirms elevated abundance in patient samples; IHC then validates spatial expression and enables scoring algorithms that can be transferred into clinical pathology workflows. This three-step paradigm is reflected in FDA guidance documents for companion diagnostic development and aligns with the evidence standards required for regulatory submission.
When designing a longitudinal IHC-based study of disease progression, pre-specifying your scoring method (H-score, Allred, manual cell counting, or digital pathology quantification) and locking down your antibody lot number before study initiation are the two most important steps to ensure data comparability across timepoints. Lot-to-lot variability in polyclonal antibody preparations is a common source of systematic error in multi-year studies.
From protocol optimization to full-slide digital scanning, professional IHC staining services can accelerate your biomarker validation pipeline. Get expert support for FFPE tissue processing, antigen retrieval optimization, and automated staining runs.
The most persistent source of confusion among researchers entering the field of tissue-based protein detection is the overlapping, inconsistently used terminology across IHC methods. The abbreviations IHC, ICC, IF, and ISH each denote distinct techniques, yet they are routinely conflated in protocols, publications, and reagent datasheets. Here is a precise reference to distinguish each method.
Detection of proteins in histologically processed tissue sections (FFPE or frozen). Preserves tissue architecture. Chromogenic or fluorescent readout. The definitive method for in situ protein localization in pathology.
Detection of proteins in cells (cultured monolayers, smears, aspirates) deposited on slides. No surrounding tissue architecture. Sample preparation is simpler than IHC but extracellular matrix context is lost. Interchangeable with IF in many lab contexts.
Fluorophore-tagged antibody detection on tissue or cells. Can be performed as IHC (IF on tissue = IHC fluorescence) or ICC. Enables multiplexing and quantitative fluorescence intensity measurement. Requires fluorescence microscope; susceptible to autofluorescence in aged FFPE.
Detection of nucleic acids (mRNA, DNA) rather than protein in tissue sections using complementary probe hybridization. Cannot directly detect protein, but mRNA expression often correlates with protein levels. FISH (fluorescent probes) and RNAscope (signal-amplified RNA ISH) are subtypes.
| Question | IHC | ICC | IF | ISH |
|---|---|---|---|---|
| Is it a type of immunohistochemistry? | Yes (it is IHC) | No (cell-based) | Can be (IF on tissue) | No (nucleic acid) |
| Detects protein? | Yes | Yes | Yes | No (mRNA/DNA) |
| Requires fluorescence microscope? | No (brightfield) | Not always | Yes | Depends (FISH yes) |
| Tissue architecture preserved? | Yes | No | If on tissue sections | Yes |
| Multiplexing capacity | 1–2 (chromogen) | 3–5 (fluorophore) | 4–40+ (panel) | 2–4 (probes) |
When performed on tissue sections, yes: immunofluorescence is a subset of immunohistochemistry that uses fluorophore-conjugated antibodies instead of enzyme-chromogen pairs. When performed on cultured cells or suspension preparations, it is technically immunocytochemistry (ICC). The term immunostaining is the broadest umbrella covering all antibody-based staining regardless of detection mode or sample type.
What are the different types of immunohistochemical stains and their specific uses?
Immunohistochemical stains are broadly categorized by their detection mode and target. Chromogenic IHC uses enzyme substrates: DAB (3,3'-diaminobenzidine) produces a permanent brown precipitate used for most routine diagnostic staining; AEC (3-amino-9-ethylcarbazole) produces a red, alcohol-soluble precipitate useful when tissues have endogenous brown pigment; FastRed and Permanent Red are alkaline phosphatase substrates used in double-staining to contrast with DAB.
Fluorescent IHC (IHC fluorescence) uses fluorophore-conjugated antibodies. FITC (green), Cy3/TRITC (red), Cy5 (far red), and Opal dyes (520, 570, 620, 690, 780 nm) are common choices for multiplex panels. Each is selected based on spectral separation, available filter sets on your microscope, and the autofluorescence background of your tissue.
By target type, immunohistochemical stains include: lineage markers (CK7, CK20, Vimentin for tumor classification), proliferation markers (Ki-67), apoptosis markers (cleaved caspase-3), immune cell markers (CD3, CD4, CD8, CD68, FoxP3), receptor markers (ER, PR, HER2, EGFR), and pathway markers (pAKT, pERK, pS6 for signaling status).
What are the advantages and disadvantages of IHC over immunofluorescence?
Immunohistochemistry vs immunofluorescence advantages (IHC): Chromogenic IHC slides are permanent, can be archived for decades, and are read under standard brightfield microscopy available in any pathology department. There is no photobleaching, the hematoxylin counterstain preserves simultaneous morphological assessment, and automated staining platforms developed for IHC have extensive regulatory validation for clinical use. IHC is also more robust in FFPE tissues with high autofluorescence (e.g., liver, lung, adipose).
Immunofluorescence advantages over IHC: IF permits 4–40+ target multiplexing on a single section through spectral separation of fluorophores. It offers quantitative fluorescence intensity data per cell amenable to image analysis pipelines. IF enables precise subcellular co-localization analysis (e.g., nuclear vs. cytoplasmic partitioning of a transcription factor) and is the backbone of emerging spatial proteomics platforms. For researchers who can invest in fluorescence imaging infrastructure, multiplex IF provides substantially richer biological data per section than single or double chromogenic IHC.
How does the principle of immunohistochemistry apply to cancer diagnosis and treatment?
The immunohistochemistry principle—that specific antibodies bind to their target antigens within morphologically preserved tissue—underpins a substantial proportion of modern cancer diagnostics. In routine surgical pathology, IHC panels are used to classify tumor histology (e.g., carcinoma vs. lymphoma vs. sarcoma), determine primary site in cancers of unknown primary using markers such as CK7, CK20, TTF-1, CDX2, PSA, and WT1, and grade tumors based on proliferative index (Ki-67).
For treatment selection, validated IHC tests are companion diagnostics: HER2 (breast, gastric cancer), ER/PR (breast cancer), PD-L1 (lung, bladder, head and neck cancer), ALK (lung cancer), ROS1 (lung cancer), and MMR/MSI proteins (colorectal, endometrial cancer) are all measured by IHC as direct determinants of therapy eligibility. An IHC test positive result for PD-L1 above a defined CPS or TPS threshold determines eligibility for pembrolizumab in multiple tumor types. An IHC test negative result for MMR proteins (MLH1, MSH2, MSH6, PMS2) indicates mismatch repair deficiency, predicting microsatellite instability and response to checkpoint inhibitor therapy.
What is the protocol for immunohistochemistry on frozen tissue sections?
The immunohistochemistry protocol for frozen sections differs from FFPE in several key steps. Fresh tissue is embedded in OCT (optimal cutting temperature) compound and snap-frozen in liquid nitrogen or a cryostat chamber. Sections are cut at 5–10 μm on a cryostat and mounted on charged glass slides.
Fixation of frozen sections is performed post-sectioning rather than before embedding. Common fixatives include 4% paraformaldehyde (10–20 min at RT), acetone (-20°C, 10 min), or methanol (-20°C, 10 min) depending on the target antigen and antibody requirements. Coagulant fixatives (acetone, methanol) are gentler on epitopes but provide less morphological detail. Antigen retrieval is usually not required for frozen sections because crosslinking has not occurred, which is the primary advantage for labile or conformational epitopes.
After fixation, the protocol proceeds similarly to FFPE IHC: endogenous peroxidase block (3% H2O2, 5–10 min), serum block (30 min), primary antibody (1 hr RT or overnight 4°C), secondary antibody and detection system, chromogen development, and counterstain. Slides should not be dewaxed (no xylene step) and rehydration is replaced by a brief wash series.
How does immunohistochemistry differ from immunocytochemistry in methodology and application?
The methodological difference between IHC and ICC begins with the sample. IHC is performed on tissue sections where the three-dimensional architecture of the organ is preserved: you can observe protein expression in the context of tumor glands, stromal compartments, vascular walls, and infiltrating immune cells. ICC is performed on cells—either cultured monolayers grown on glass coverslips or cell suspensions (blood smears, cytology aspirates, bronchoalveolar lavage) deposited on slides. No surrounding extracellular matrix remains.
This fundamental difference dictates where each method is applied: IHC for tissue biomarker studies, cancer diagnosis, and in vivo target validation; ICC for in vitro mechanistic studies, drug response assays in cell lines, and intracellular signaling pathway analysis where the cell is the unit of analysis rather than the tissue. ICC samples typically require a cell permeabilization step (Triton X-100 or saponin) to permit antibody access to intracellular antigens, whereas many IHC protocols achieve permeabilization inherently through the antigen retrieval step.
In terms of antibody protocols, most antibody clones validated for IHC are also applicable to ICC, but optimal concentrations and incubation conditions differ due to differences in sample thickness, fixation depth, and background signal sources. Many labs refer to IF staining of cells as "ICC/IF" and IF staining of tissue as "IHC/IF," which contributes to the terminology confusion addressed in Section 10.