This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
and ELISA kits, proteins related to fibrosis biology, extracellular matrix remodeling, and tissue scarring.
Fibrosis research focuses on how chronic injury, inflammation, and failed tissue repair drive excessive extracellular matrix deposition and permanent scarring across organs such as the lung, liver, kidney, heart, and skin. Antibodies are essential tools in fibrosis studies because they enable researchers to track fibroblast activation, epithelial injury, immune remodeling, matrix accumulation, and pro-fibrotic signaling in tissues, cell models, and biofluids. In histology-driven workflows, IHC and IF help localize collagens, periostin, α-SMA, osteopontin, and epithelial injury markers within fibrotic lesions. In mechanistic studies, Western blot supports pathway readouts such as TGF-β/Smad, PI3K/Akt, hypoxia, EMT, and matrix remodeling. ELISA and multiplex assays are commonly used to quantify soluble mediators including IL-6, CCL18, TGF-β-related factors, and other circulating fibrosis-associated proteins. This fibrosis antibodies hub is designed to help researchers navigate fibrosis biomarkers, organ-specific disease contexts, relevant cell types, and signaling pathways so they can more quickly identify validated antibodies and assays for IHC/IF, ELISA, and Western blot applications.
Fibrosis biomarker panels typically combine matrix proteins, epithelial injury markers, inflammatory mediators, and signaling regulators to capture both disease activity and mechanism. Common readouts include collagen deposition, fibroblast activation, TGF-β pathway activity, alveolar epithelial stress, and immune-driven remodeling.

Anti-Collagen I/COL1A1 Antibody Picoband®, Figure 5.
IF analysis of COL1A1 using anti-COL1A1 antibody (PA2140-1).
COL1A1 was detected in a paraffin-embedded section of human endom...

Anti-Collagen I/COL1A1 Antibody Picoband®, Figure 2.
IHC analysis of COL1A1 using anti COL1A1 antibody (PB9939).
COL1A1 was detected in a paraffin-embedded section of...
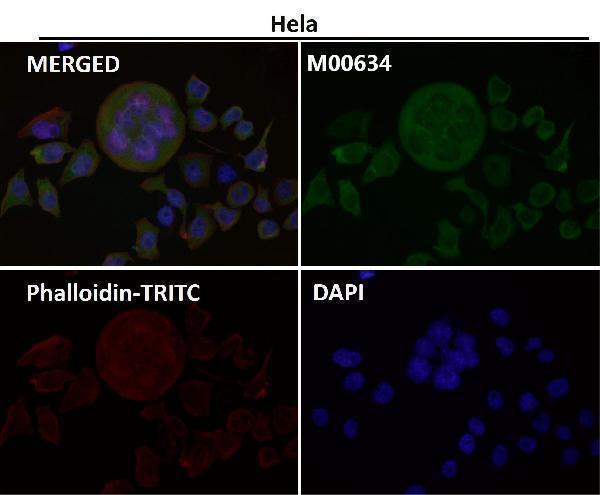
Anti-Osteopontin SPP1 Rabbit Monoclonal Antibody, Immunofluorescent analysis using the Antibody at 1:150 dilution....
| Protein Name | Gene Name | Function |
|---|---|---|
| Mucin 5B | MUC5B | Variant associated with susceptibility to idiopathic pulmonary fibrosis |
| Transforming Growth Factor Beta 1 | TGFB1 | Promotes fibrosis by stimulating extracellular matrix production |
| Matrix Metalloproteinase 7 | MMP7 | Involved in extracellular matrix remodeling |
| Surfactant Protein C | SFTPC | Important for lung function; mutations linked to pulmonary fibrosis |
| Surfactant Protein A | SFTPA1 | Roles in innate immunity and lung homeostasis |
| Krebs von den Lungen 6 (KL-6) | MUC1 | Marker for interstitial lung disease activity |
| Periostin | POSTN | Involved in tissue remodeling and fibrosis |
| CC-chemokine ligand 18 | CCL18 | Associated with fibrosis progression |
| Osteopontin | SPP1 | Involved in cell adhesion and migration |
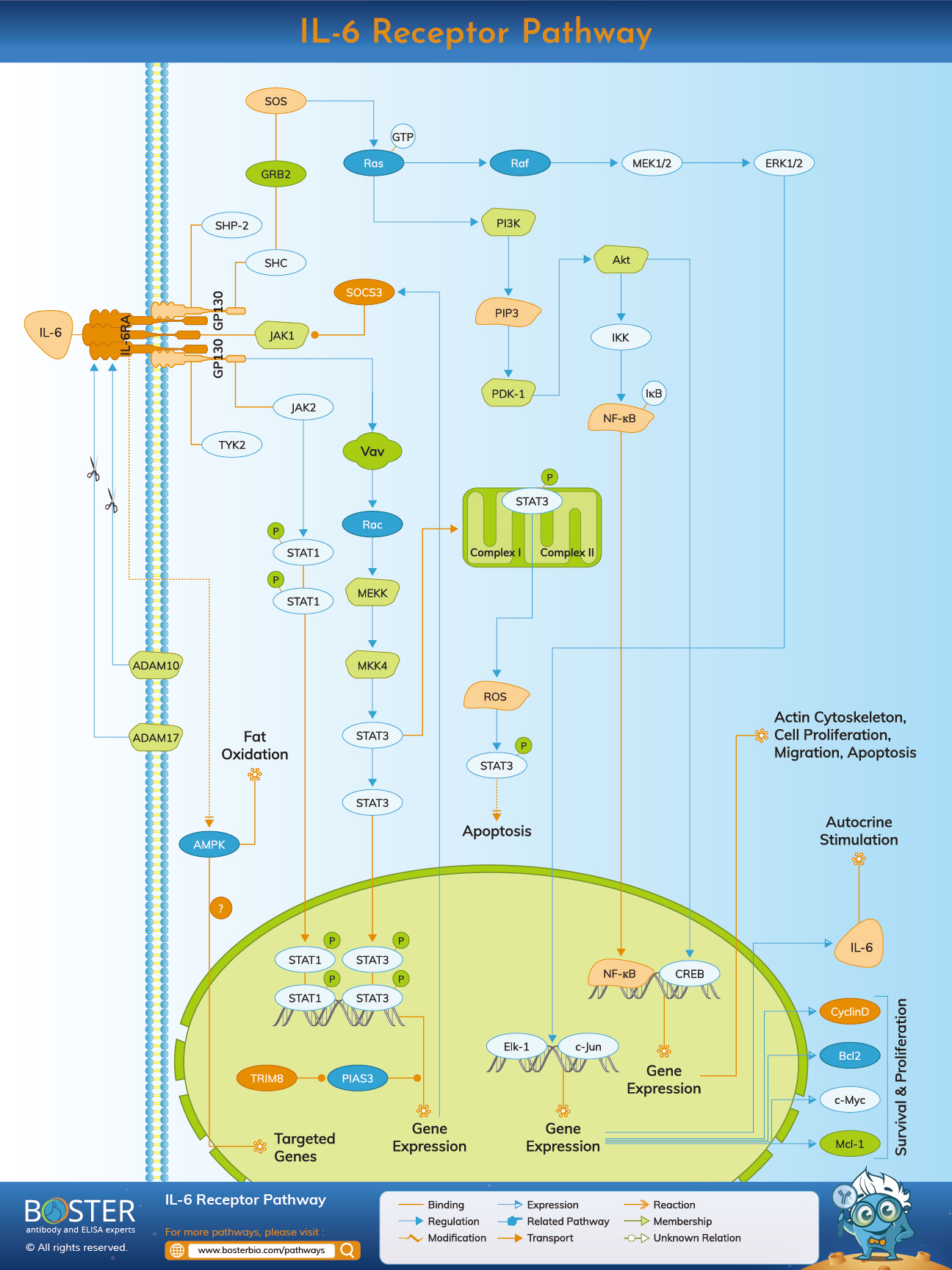
| Interleukin 6 | IL6 | Pro-inflammatory cytokine linked to fibrosis |
| Fibroblast Growth Factor 2 | FGF2 | Involved in cell growth and differentiation |
| Integrin alpha-V | ITGAV | Mediates cell-matrix interactions in fibrosis |
| Interleukin 13 | IL13 | Promotes fibrosis through immune modulation |
| Epithelial Growth Factor | EGF | Regulates cell growth and differentiation |
| Elastin | ELN | Provides elasticity to lung tissue; remodeling involved in fibrosis |
| Collagen Type I | COL1A1 | Major component of extracellular matrix in fibrosis |
| Collagen Type III | COL3A1 | Contributes to extracellular matrix structure |
| Transforming Growth Factor Beta Receptor II | TGFBR2 | Mediates TGF-beta signaling in fibrosis |
Localize collagen deposition, epithelial injury, fibroblast activation, and immune cell remodeling directly in fibrotic tissue. IHC and IF are core methods for studying lesion architecture and cell-type-specific expression patterns across lung, liver, kidney, heart, and skin fibrosis models.
Explore IHC/IF assay guideQuantify secreted fibrosis-associated factors such as IL-6, TGF-β-related mediators, chemokines, and remodeling proteins in serum, BALF, culture supernatant, or tissue lysate. ELISA is especially useful for longitudinal studies and translational readouts.
Explore ELISA assay guideConfirm activation of TGF-β/Smad, PI3K/Akt, hypoxia, EMT, and matrix remodeling pathways. Western blot is widely used to compare fibroblast activation, epithelial stress, and treatment response in mechanistic fibrosis studies.
Explore Western blot guideProfile macrophages, lymphocytes, epithelial populations, and activated stromal cells in fibrotic tissues. Flow cytometry helps resolve inflammatory-to-fibrotic transitions and supports cell-state analysis in disease and drug-response models.
Explore flow cytometry guideLung fibrosis research often focuses on alveolar epithelial stress, abnormal wound healing, myofibroblast expansion, collagen deposition, and inflammatory remodeling. Common readouts include TGF-β signaling, osteopontin, periostin, surfactant proteins, mucins, and extracellular matrix markers measured across tissue sections, BALF, and cell models.
Some fibrosis programs emerge in systemic disease settings where inflammation, vascular injury, and persistent repair signaling promote widespread matrix remodeling. These models are especially relevant for studying fibroblast-immune crosstalk, cytokine signaling, endothelial dysfunction, and tissue stiffening across multiple compartments.
Fibrosis biology also overlaps with chronic remodeling in the liver, kidney, and cardiovascular system, where extracellular matrix accumulation, inflammatory signaling, hypoxia, and endothelial dysfunction contribute to tissue dysfunction. These disease areas provide useful comparative contexts for broader fibrosis-focused marker panels and pathway studies.
Activated fibroblasts and myofibroblasts are central drivers of fibrotic remodeling because they produce collagens, periostin, fibronectin, and other extracellular matrix components while responding to TGF-β, integrins, and mechanical stress. These cells are often profiled together with endothelial and epithelial compartments to define lesion stage and therapeutic response.
Injured epithelial cells shape the fibrotic microenvironment by releasing danger signals, cytokines, and growth factors that recruit immune cells and activate fibroblasts. EMT-related programs, altered differentiation states, and impaired regeneration are therefore important contexts when interpreting fibrosis biomarkers in tissue and in vitro systems.
Macrophages, lymphocytes, and other immune cells influence fibrosis by regulating cytokine production, growth factor release, matrix turnover, and tissue repair programs. These immune compartments are particularly relevant when studying disease progression, inflammatory-to-fibrotic transitions, and therapeutic intervention.
Central pathways that regulate fibroblast activation, extracellular matrix production, and persistent scar formation.
Pathways that connect epithelial injury, cell-state transition, extracellular matrix remodeling, and persistent scar architecture.
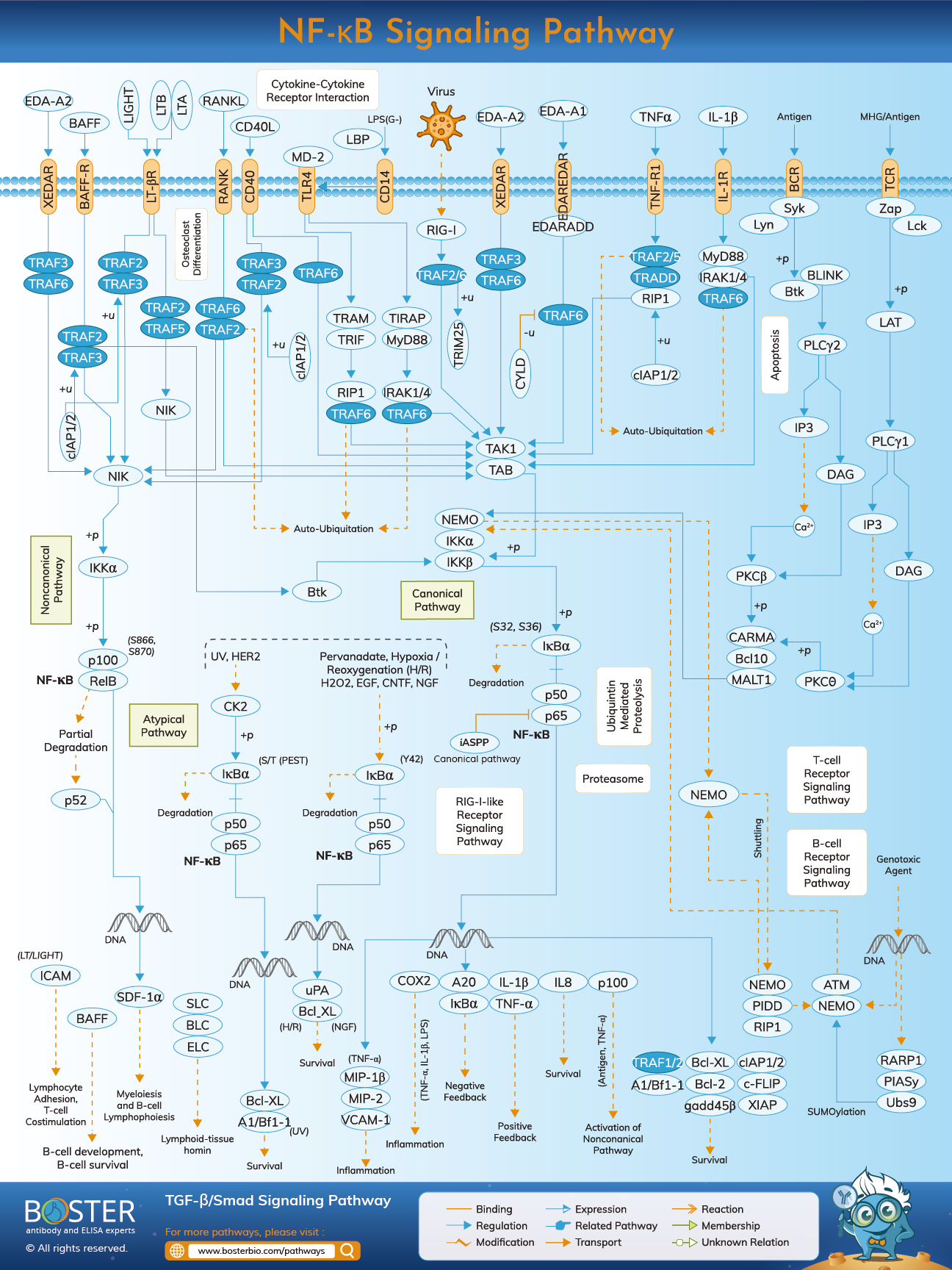
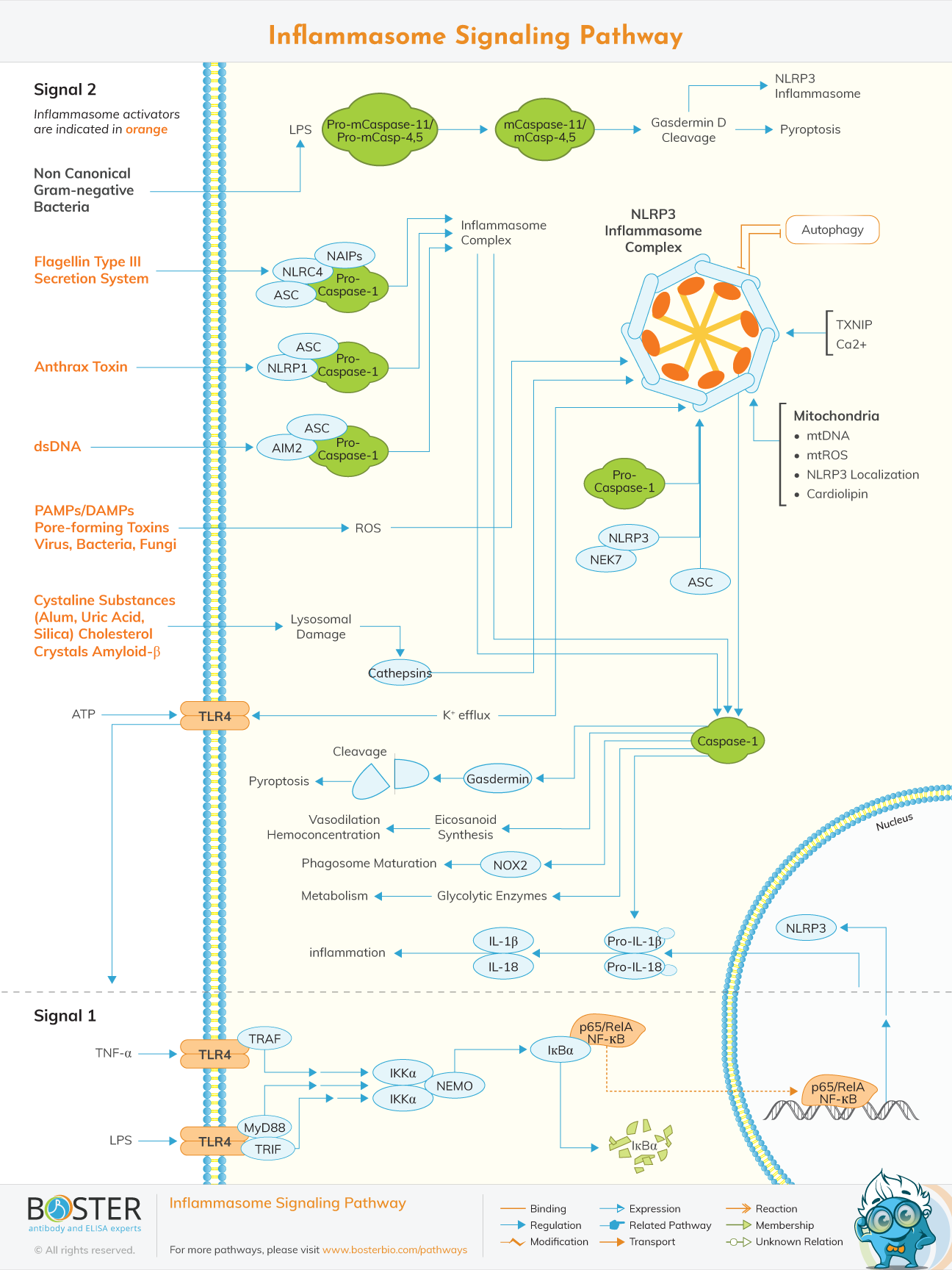
Inflammatory and stress-associated pathways that shape fibroblast-immune crosstalk and chronic tissue remodeling.
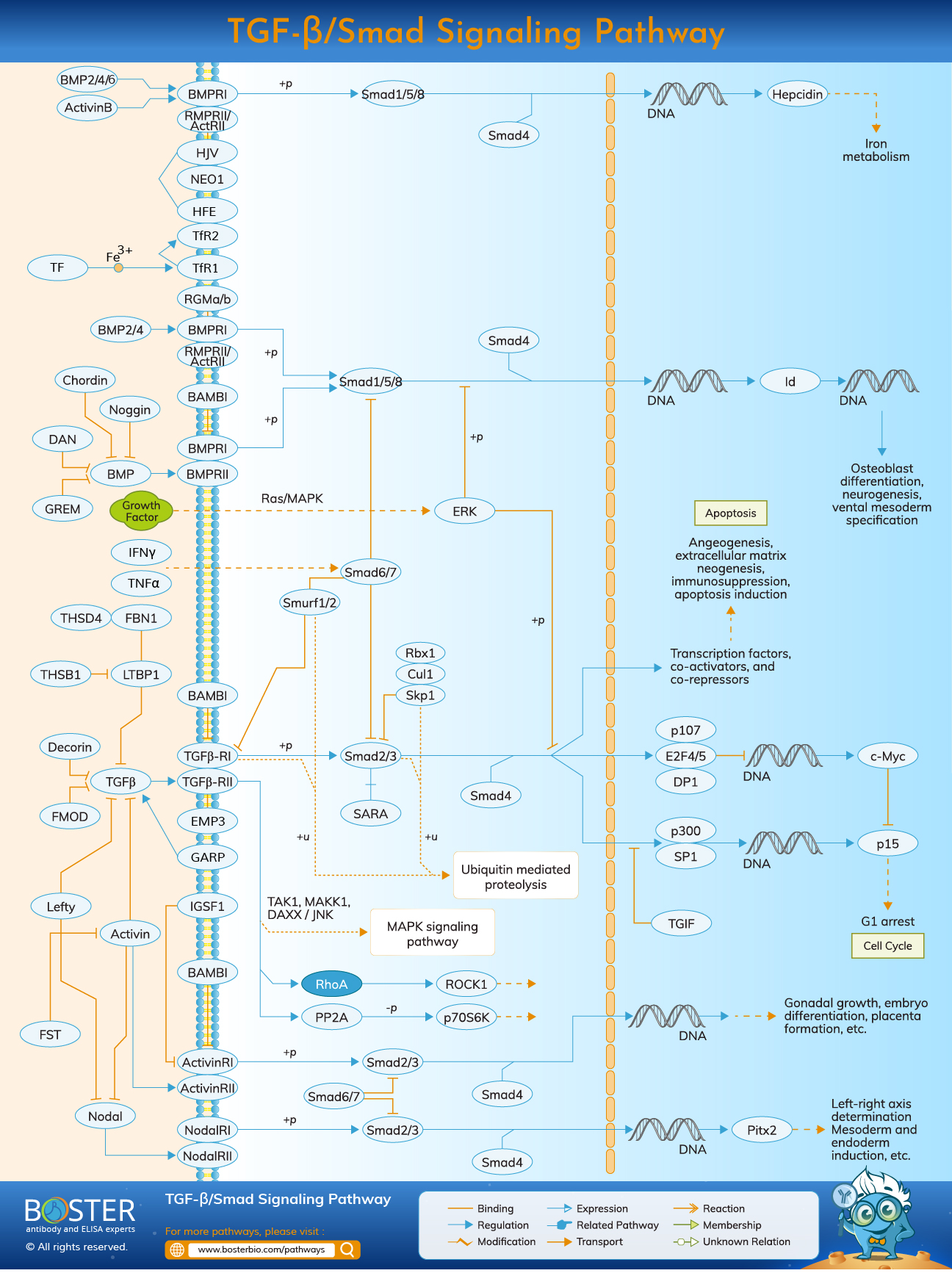
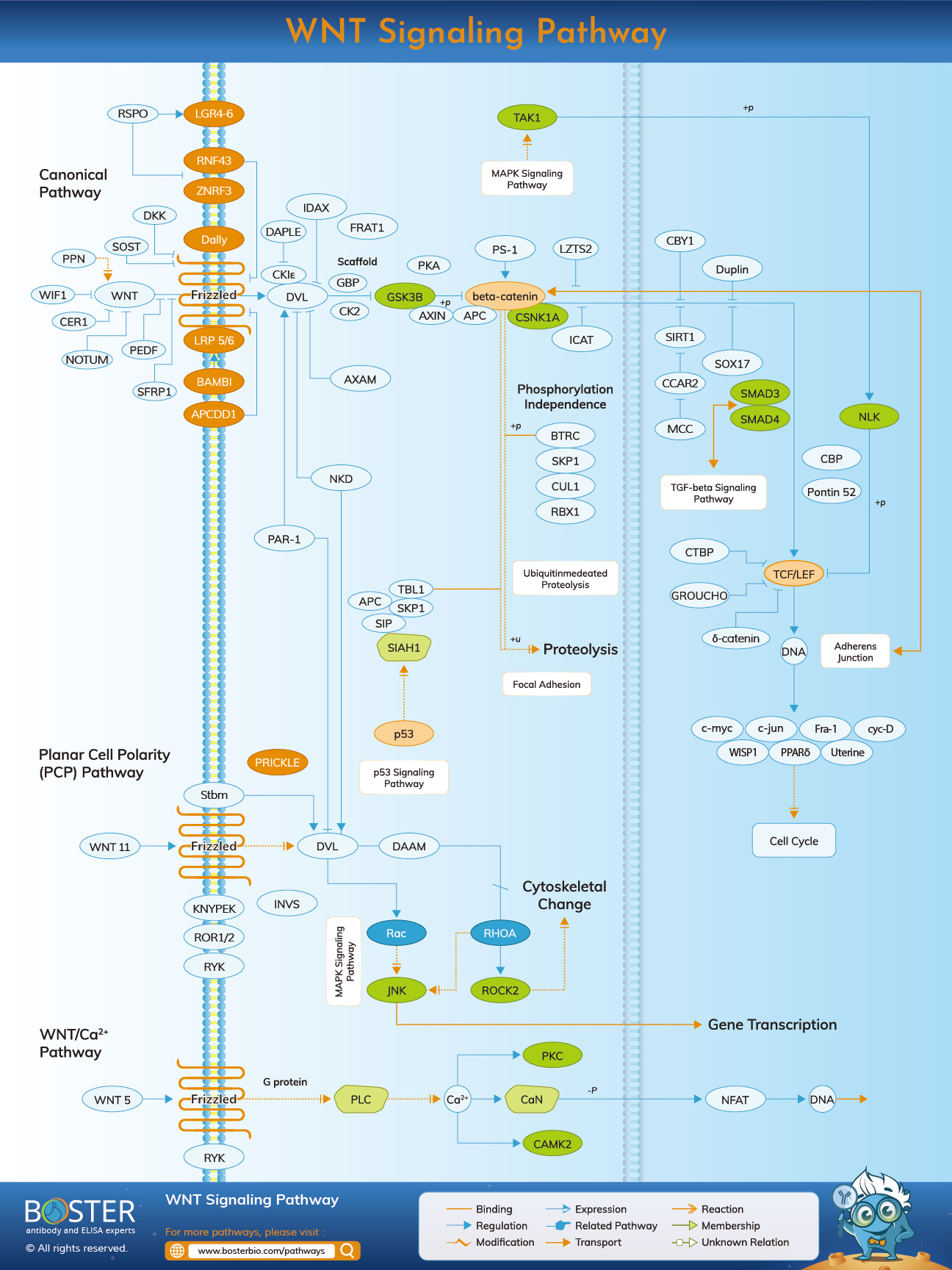
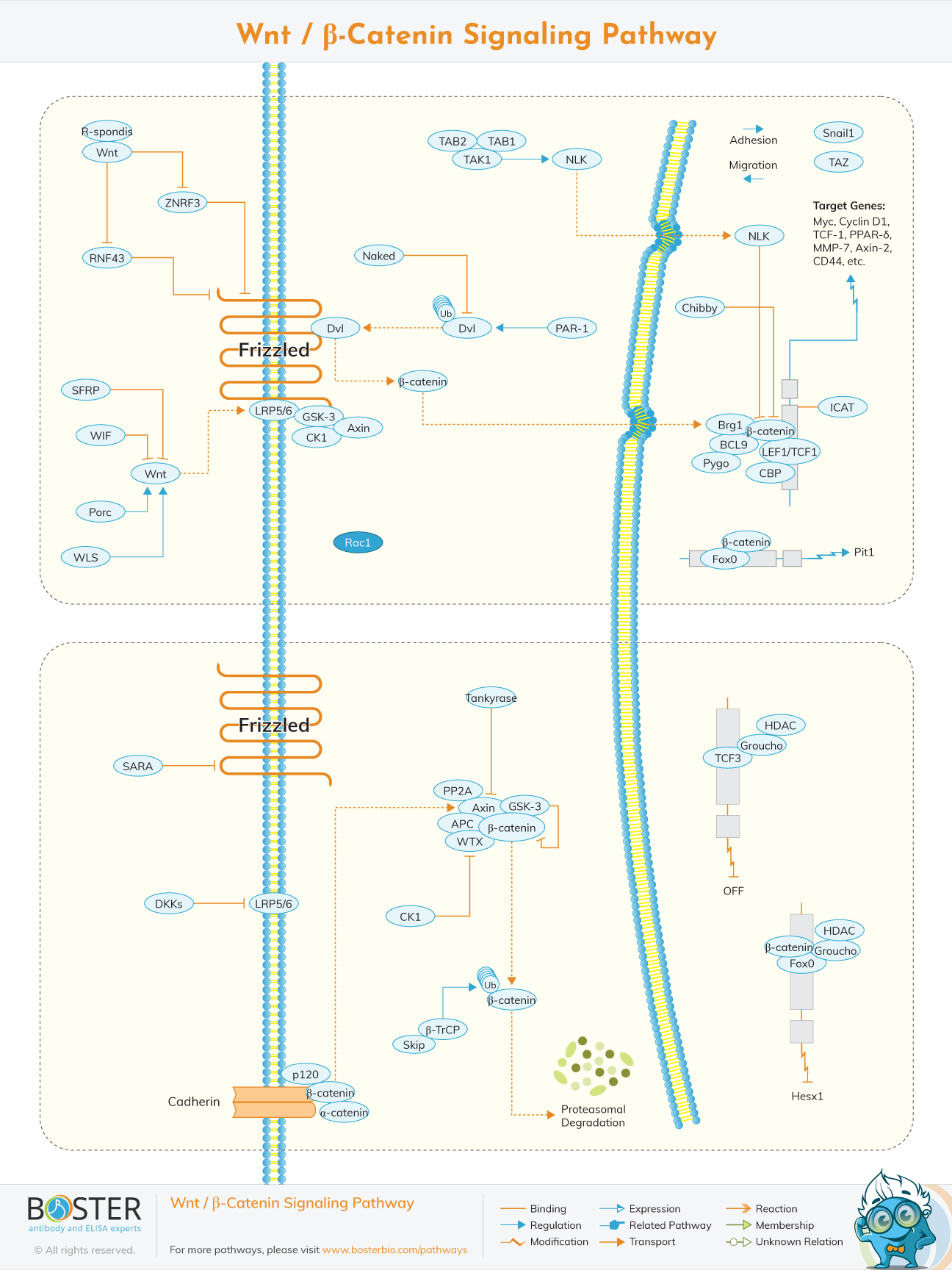
The Transforming Growth Factor-beta (TGF-β) signaling pathway is one of the central drivers of fibrosis across multiple organs. TGF-β promotes fibroblast activation, myofibroblast differentiation, extracellular matrix accumulation, and tissue stiffening, making it a core pathway in pulmonary fibrosis and broader fibrosis biology. In fibrotic tissues, elevated TGF-β activity supports collagen deposition, periostin expression, integrin-mediated signaling, and persistent remodeling programs that fail to resolve after injury. Because TGF-β signaling also intersects with pathways such as PI3K/Akt, hypoxia, and Wnt/β-catenin, it is often studied as a mechanistic hub rather than an isolated pathway. Antibody-based readouts of TGFB1, TGFBR2, downstream effectors, and matrix proteins are therefore widely used to profile disease state and treatment response in fibrosis models.
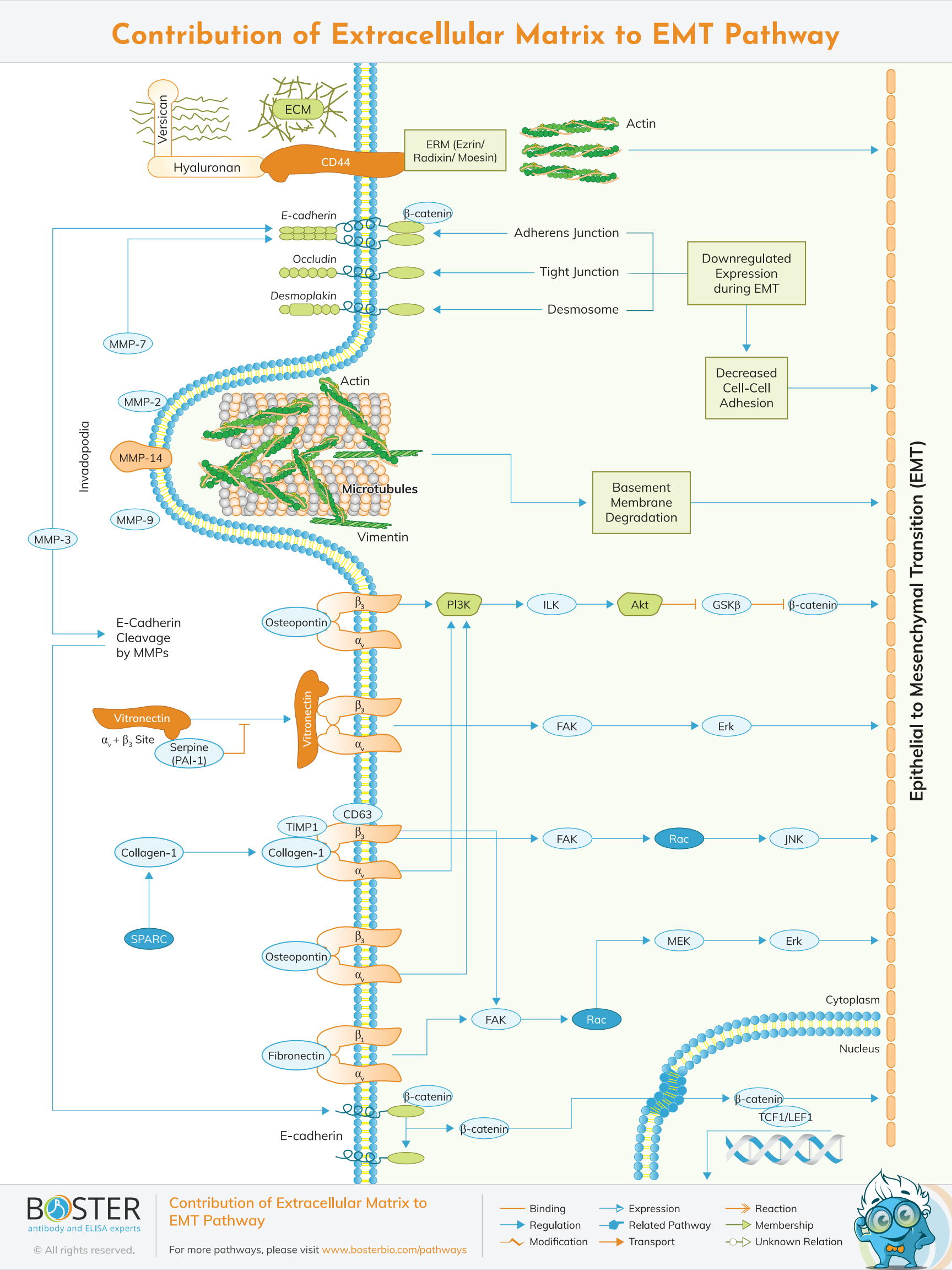
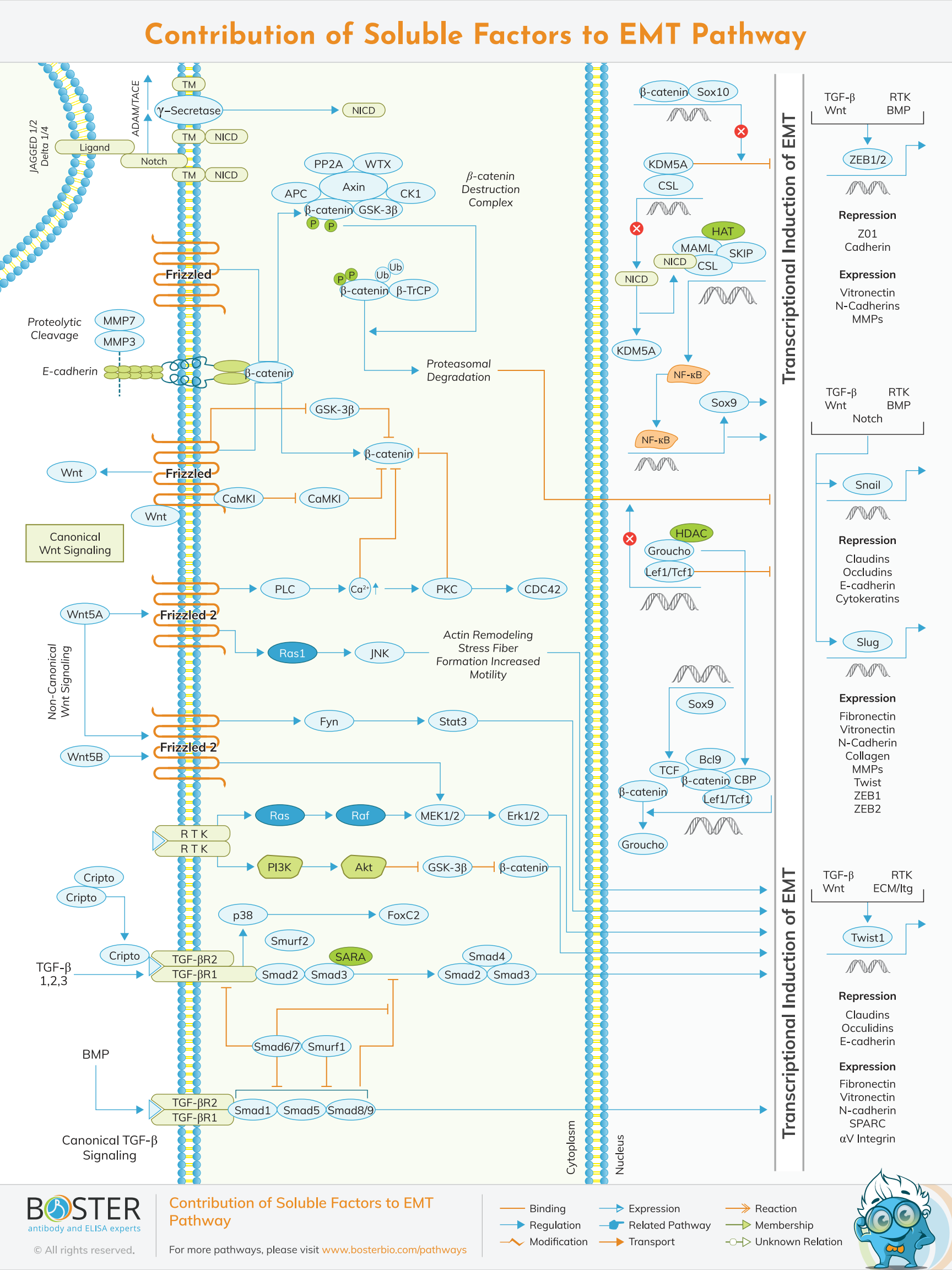
Fibrosis often begins with persistent epithelial stress and abnormal repair, particularly in barrier tissues such as the lung. Injured epithelial cells can release pro-fibrotic mediators, alter differentiation programs, and contribute to a microenvironment that favors fibroblast activation and matrix remodeling. EMT-related signaling is frequently studied in this context because it captures the transition from epithelial stability toward mesenchymal-like phenotypes associated with migration, loss of polarity, and fibrotic signaling. Although the degree of direct epithelial contribution to fibroblast pools may vary by model, EMT-associated markers remain highly informative for interpreting disease activity, epithelial dysfunction, and tissue remodeling. Antibodies against epithelial markers, osteopontin, periostin, collagens, and signaling mediators help connect epithelial injury to downstream fibrosis mechanisms.
The defining pathological feature of fibrosis is excessive extracellular matrix deposition combined with abnormal tissue remodeling. Activated fibroblasts and myofibroblasts produce collagens, elastin-associated remodeling proteins, periostin, and other matrix components that alter tissue mechanics and sustain scar formation. Matrix remodeling enzymes, integrin signaling, inflammatory cytokines, and mechanical stress all reinforce this process, creating a feed-forward loop that is difficult to reverse once established. This is why fibrosis workflows frequently combine matrix markers such as COL1A1, COL3A1, ELN, POSTN, and MMP7 with pathway and immune readouts to build a more complete view of lesion progression and therapeutic effect.