This website uses cookies to ensure you get the best experience on our website.
- Table of Contents
and ELISA kits, proteins related to cancer biology.
Cancer research investigates how normal cells acquire malignant traits such as uncontrolled proliferation, resistance to cell death, invasion, metastasis, and immune evasion. Antibodies are essential tools in this field because they enable specific detection of tumor biomarkers, oncogenic signaling nodes, and tumor microenvironment (TME) components across tissues and model systems. In pathology and translational studies, IHC and IF help localize markers (e.g., cytokeratins, Ki-67, HER2, PD-L1) in the spatial context of tumors. In mechanistic work, Western blot supports pathway readouts (MAPK/ERK, PI3K/AKT, apoptosis and DNA damage). Flow cytometry enables deep immune and tumor cell phenotyping, while ELISA and multiplex assays quantify soluble mediators such as cytokines, growth factors and circulating biomarkers. This cancer antibodies hub is designed to help you navigate cancer by experimental approach and tumor type, and to quickly select validated antibodies and assays for IHC/IF, flow cytometry, ELISA, and Western blot.
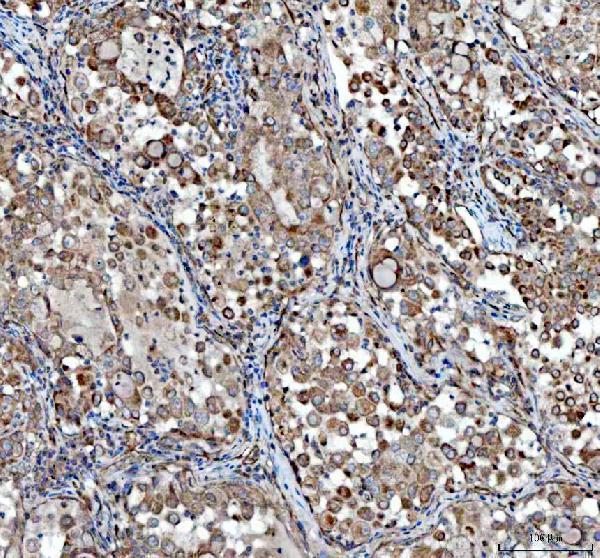
Anti-VEGF/VEGFA Antibody Picoband®, Figure 2. IHC analysis of VEGFA using anti-VEGFA antibody (PA1080).
VEGFA was detected in a paraffin-embedded section of human lung cancer tissue. Heat...
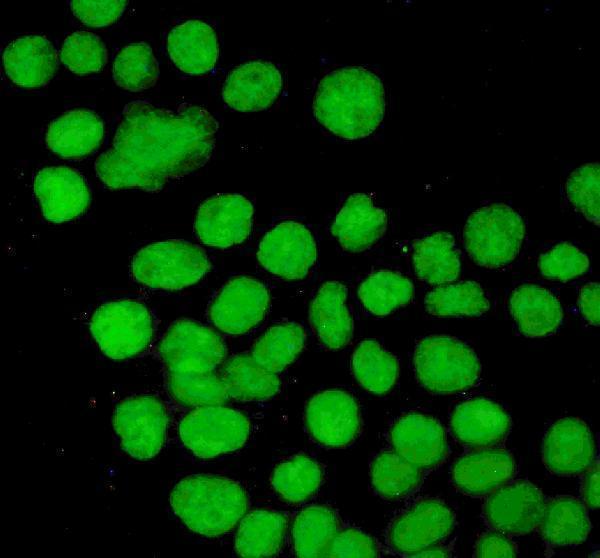
Anti-P53/TP53 Antibody Picoband®, Figure 3. IF analysis of P53 using anti-P53 antibody (PB9008).
P53 was detected in immunocytochemical section of A431 cells. Enzyme antigen...

Anti-P53 Tp53 Monoclonal Antibody, Figure 3. IF analysis of p53 using anti-p53 antibody (MA1078).
p53 was detected in immunocytochemical section of A431 cell. Enzyme antigen retrieva...
| Protein Name | Gene Name | Function |
|---|---|---|
| HER2 | ERBB2 | Promotes cell growth and differentiation; overexpression linked to aggressive breast cancer. |
| EGFR | EGFR | Regulates cell growth and survival; mutations associated with various cancers including lung and colorectal. |
| BRCA1 | BRCA1 | Involved in DNA repair; mutations increase risk of breast and ovarian cancers. |
| PD-L1 | CD274 | Suppresses the immune system; overexpression allows cancer cells to evade immune detection. |
| KRAS | KRAS | GTPase involved in cell signaling; mutations drive cancer progression in colorectal and lung cancers. |
| ALK | ALK | Tyrosine kinase receptor; rearrangements linked to non-small cell lung cancer. |
| BRAF | BRAF | Serine/threonine kinase in MAPK pathway; mutations common in melanoma. |
| MYC | MYC | Transcription factor regulating cell proliferation; overexpressed in many cancers. |
| TP53 | TP53 | Tumor suppressor involved in cell cycle regulation and apoptosis; mutations prevalent in various cancers. |
| VEGF | VEGFA | Promotes angiogenesis; targeted to inhibit tumor blood supply. |
| ER | ESR1 | Estrogen receptor; drives growth in estrogen receptor-positive breast cancers. |
| PR | PGR | Progesterone receptor; involved in hormone-driven breast cancer. |
| CTLA-4 | CTLA4 | Immune checkpoint receptor; targeted to enhance immune response against tumors. |
| ABL1 | ABL1 | Tyrosine kinase; fusion with BCR leads to chronic myeloid leukemia. |
| PIK3CA | PIK3CA | Catalytic subunit of PI3K; mutations activate the PI3K/AKT pathway in various cancers. |
| MET | MET | Receptor tyrosine kinase; implicated in tumor growth, metastasis, and angiogenesis. |
| ALK | ALK | Anaplastic lymphoma kinase; alterations associated with several cancers including lymphoma and lung cancer. |
| HER3 | ERBB3 | Receptor tyrosine kinase; dimerizes with HER2 to activate signaling pathways promoting cancer cell survival. |
| PD-1 | PDCD1 | Immune checkpoint receptor; targeted to boost immune response against tumors. |
Map tumor heterogeneity in situ: receptor status, proliferation, EMT markers, angiogenesis, and immune infiltration. IHC/IF is ideal for validating spatial biology in tumor tissue and xenograft models.
Explore IHC/IF assay guideQuantify cytokines, growth factors (e.g., VEGF), and soluble checkpoints across tumor models. Use ELISA or multiplex formats to track therapy response, inflammation, and microenvironment remodeling.
Explore ELISA assay guideProfile tumor-infiltrating lymphocytes (TILs), myeloid populations, and checkpoint expression at single-cell resolution. Build multi-color panels for immuno-oncology and TME phenotyping.
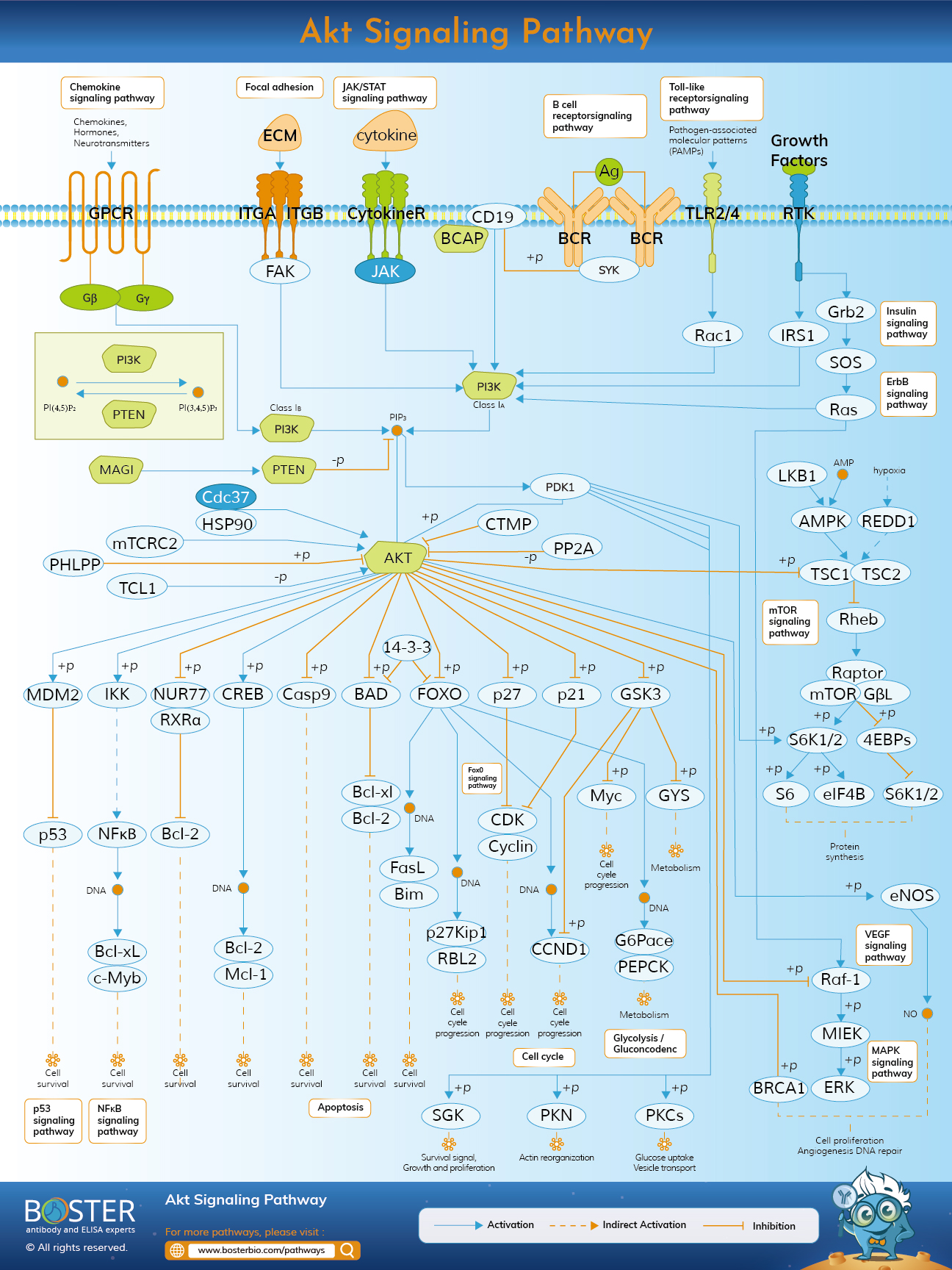
Explore flow cytometry guideConfirm activation of oncogenic pathways (MAPK/ERK, AKT/mTOR), apoptosis markers, and EMT regulators. Pair pathway antibodies with validated loading controls for tumor lysates.
Explore Western blot guideCommon solid tumors remain one of the most widely studied entry points in cancer research. Researchers often begin with biomarkers that help confirm tumor identity, distinguish subtypes, evaluate receptor status, and link expression patterns to prognosis or treatment response. These workflows frequently combine IHC or IF for tissue-level context with Western blot, ELISA, or multiplex assays for pathway and biomarker validation.
Gastrointestinal and hepatobiliary cancers are frequently studied through signaling changes linked to proliferation, invasion, inflammation, angiogenesis, and epithelial–mesenchymal transition. These tumor settings often require biomarkers that capture both tumor-cell behavior and microenvironment remodeling across IHC, IF, Western blot, ELISA, and related assay workflows.
Some cancer models are shaped by highly specific tissue context, lineage features, or treatment-response challenges. CNS tumors are closely tied to neural and glial biology, melanoma research often focuses on immune evasion and targeted-therapy response, and other specialized tumor types may require narrower biomarker panels for lineage, invasion, and tumor microenvironment analysis.
Hematologic malignancies are commonly investigated through lineage-defining markers, immune phenotype, proliferation status, and dysregulated differentiation pathways. These disease models often involve targets used in flow cytometry, Western blot, IHC, or expression profiling workflows across leukemia, lymphoma, myeloma, and bone marrow-related malignancies.
Many cancer workflows begin by defining tumor lineage and tissue context. Epithelial lineage markers support carcinoma identity and EMT studies, while CNS tumors often require neuron and glial context. Liver, adipose, and stem-like cell states can also shape tumor behavior, metastasis, and therapy response in tissue-specific models.
Cancer-associated stroma and vascular niches influence tumor growth, hypoxia, invasion, and therapy resistance. Fibroblasts and ECM remodeling help create supportive microenvironments, while endothelial cells, pericytes, smooth muscle cells, and platelets contribute to vessel structure, perfusion, metastatic seeding, and barrier function.
Immune context strongly influences tumor progression, immune escape, and treatment response. T cells and NK cells may mediate tumor killing, while macrophages, dendritic cells, neutrophils, and broader myeloid populations can shape antigen presentation, inflammation, immune suppression, and remodeling. These entry points support flow, IF/IHC, and tumor–immune interaction studies across many cancer settings.
Core oncogenic pathways that drive growth, survival, and therapy response readouts.
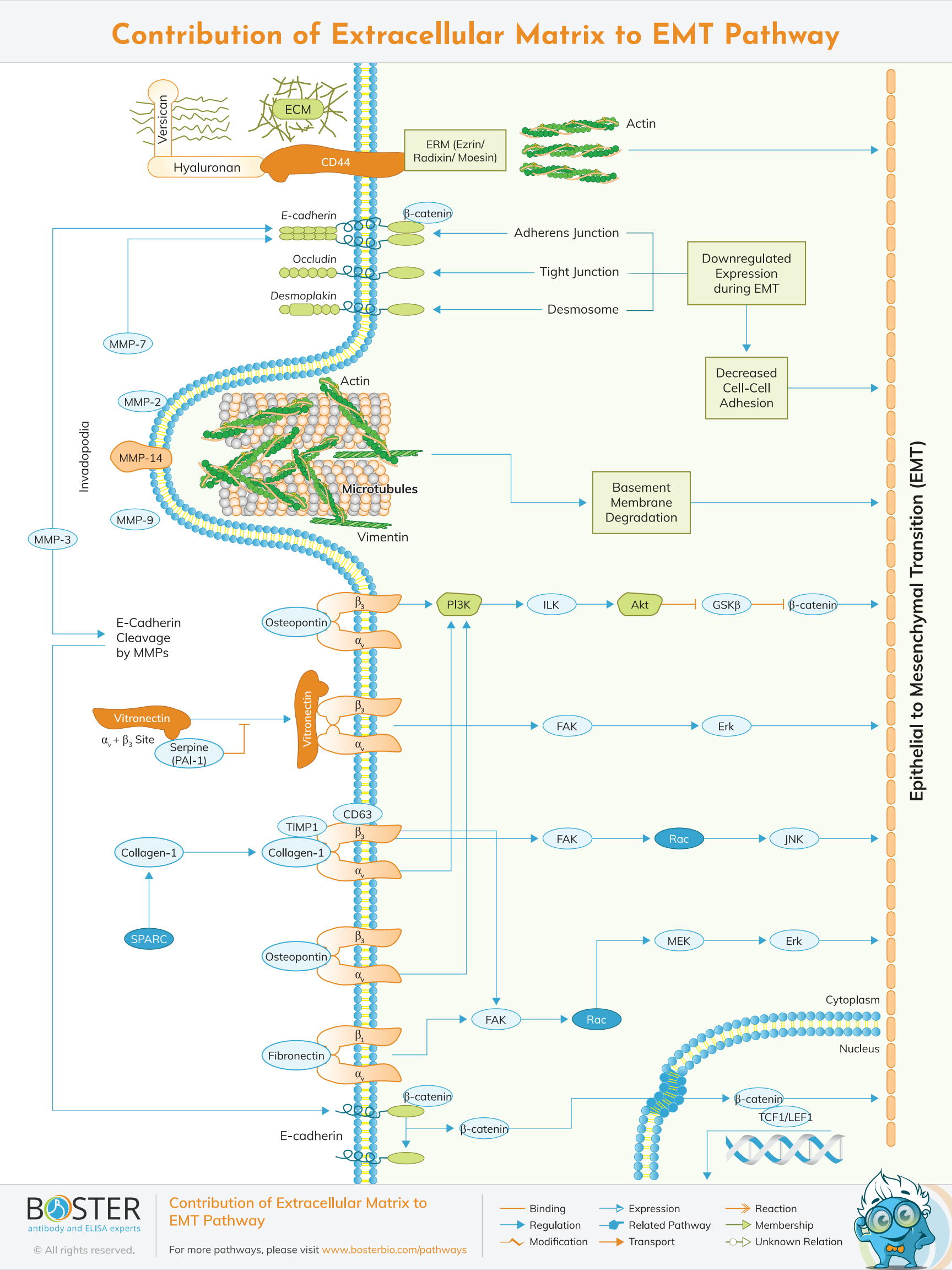
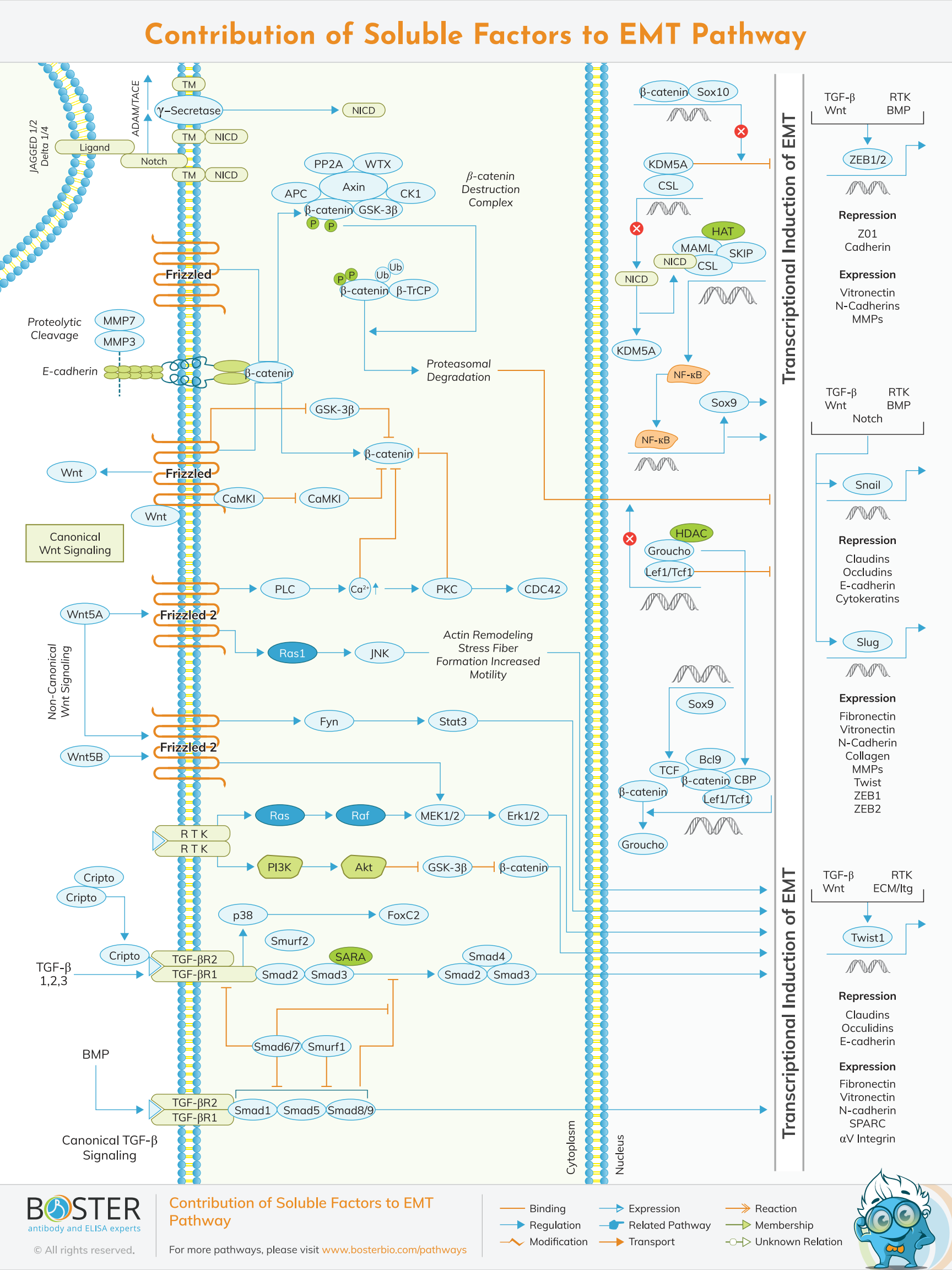
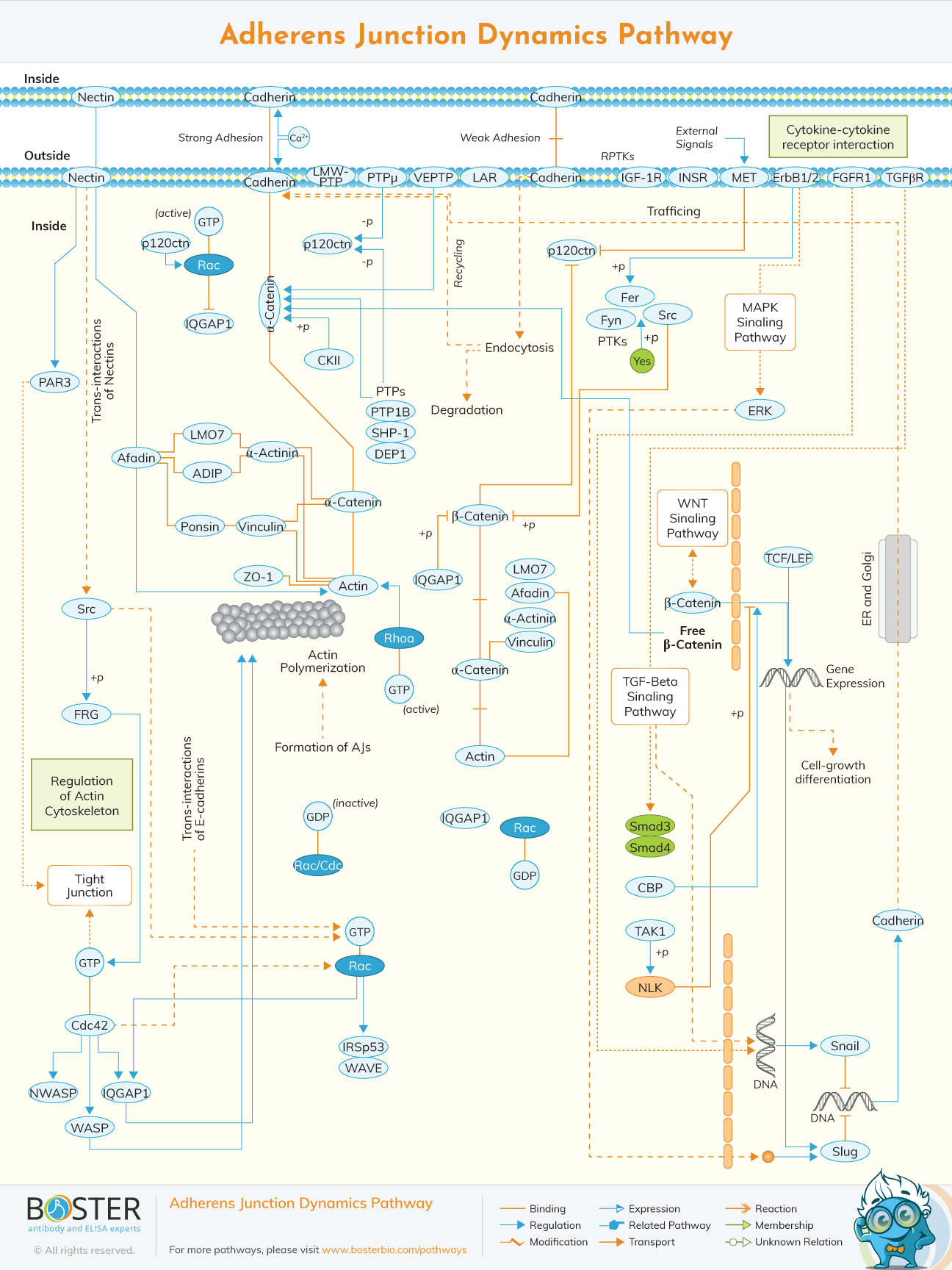
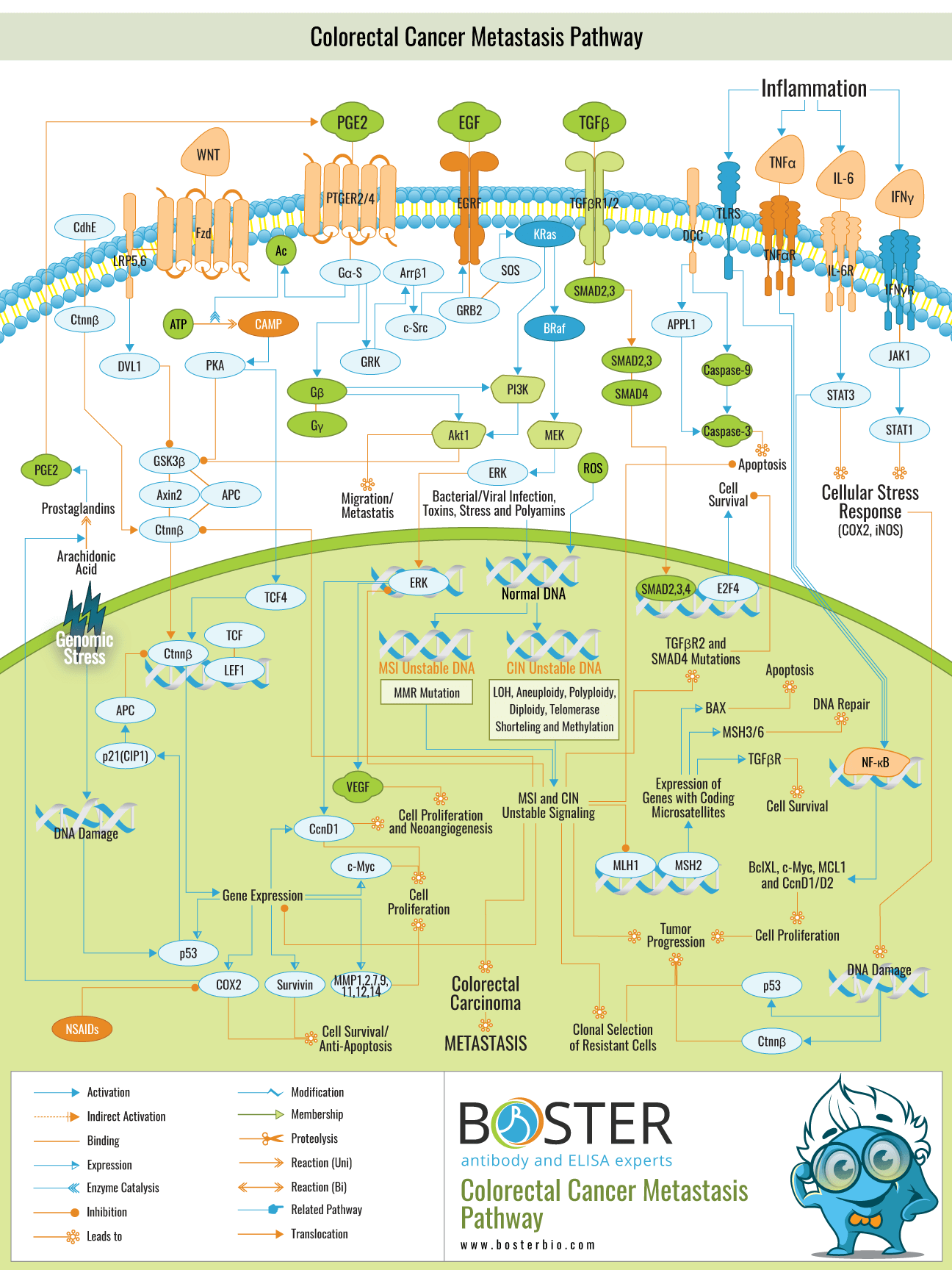
Pathways for plasticity, migration programs, and microenvironment-driven metastatic progression.
Tumor adaptation programs: metabolic rewiring, vascular remodeling, and immunotherapy-relevant escape.
Immunotherapy has emerged as a groundbreaking approach in cancer treatment, harnessing the body's own immune system to recognize and combat malignant cells. Unlike traditional therapies such as chemotherapy and radiation, which directly target cancer cells but often affect healthy tissues, immunotherapy aims to enhance the immune system's natural ability to detect and destroy cancer cells with greater specificity and reduced side effects. Key strategies within immunotherapy include checkpoint inhibitors, which block proteins that suppress immune responses, CAR T-cell therapy, which involves engineering a patient's T-cells to better target cancer cells, and cancer vaccines designed to elicit an immune response against specific tumor antigens. This sub-research area has shown remarkable success in treating various cancers, including melanoma, lung cancer, and certain types of leukemia, leading to prolonged survival rates and, in some cases, complete remission. Ongoing research seeks to overcome challenges such as immune resistance and adverse effects, while expanding the efficacy of immunotherapy across a broader spectrum of malignancies.
The tumor microenvironment (TME) refers to the complex milieu surrounding a tumor, comprising various cell types, signaling molecules, and structural components that interact with cancer cells. Understanding the TME is crucial, as it plays a pivotal role in tumor growth, progression, metastasis, and response to therapy. Key components of the TME include immune cells, fibroblasts, blood vessels, extracellular matrix, and signaling molecules such as cytokines and growth factors. These elements can either suppress or promote tumor development, depending on the context. For instance, cancer-associated fibroblasts can facilitate tumor expansion and resistance to treatment, while certain immune cells within the TME may either attack the tumor or be co-opted to support its growth. Research in this area focuses on deciphering the intricate interactions within the TME to identify novel therapeutic targets and strategies. By modulating the TME, scientists aim to inhibit tumor progression, enhance the efficacy of existing treatments like immunotherapy, and prevent metastasis, ultimately leading to improved patient outcomes.